
Neonatal Fetal Nutrition & Metabolism 2
Session: Neonatal Fetal Nutrition & Metabolism 2
 photo")
Isaura Molina Stornelli, MD (she/her/hers)
Neonatologist
Ochsner Medical Center
Flushing Hospital Medical Center
Metairie, Louisiana, United States
.png)
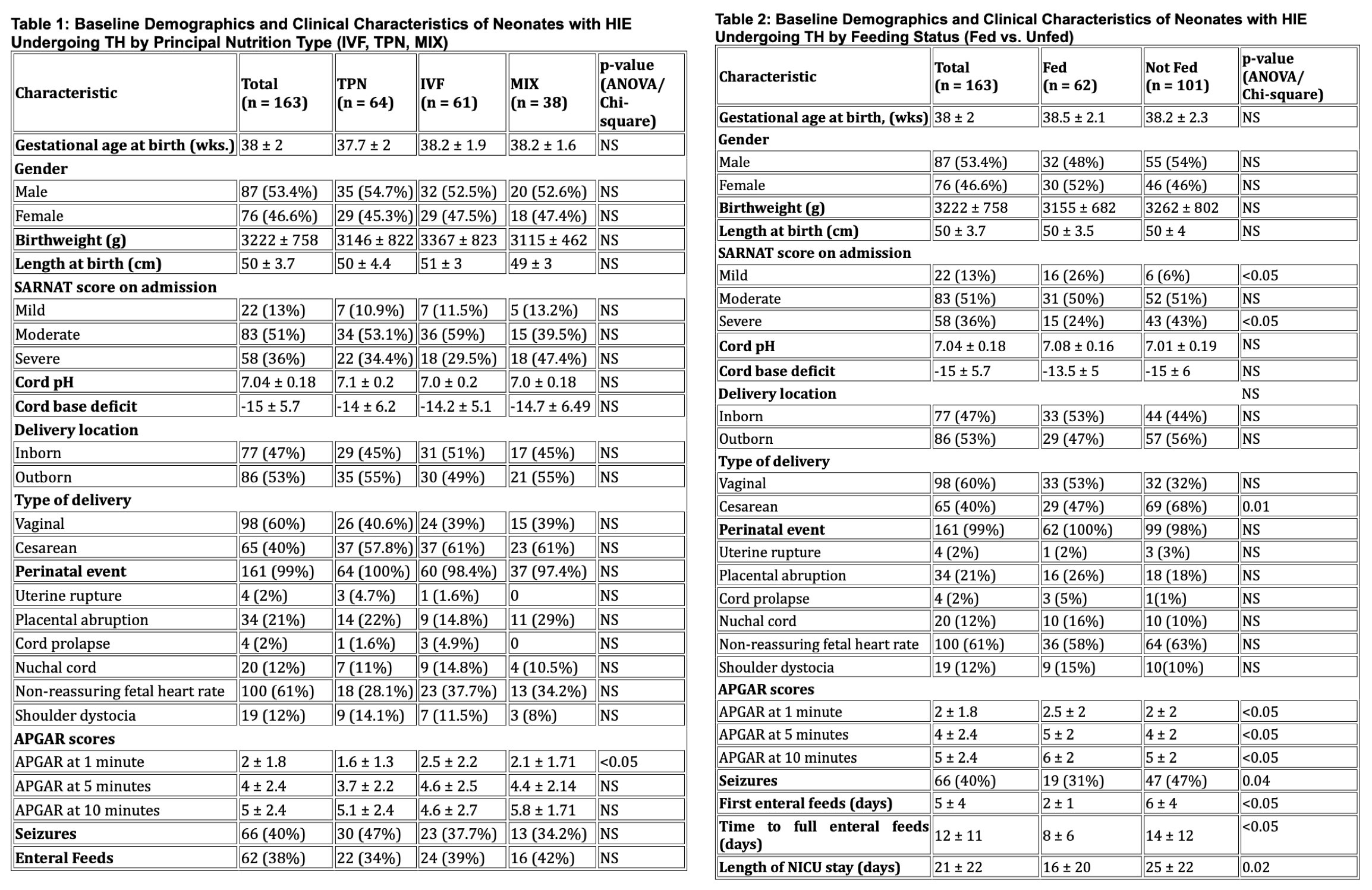 Table 1: By Principal Nutrition Type (IVF, TPN, MIX)
Table 1: By Principal Nutrition Type (IVF, TPN, MIX)