
General Pediatrics 4
Session: General Pediatrics 4
 photo")
Grace Truong, MD (she/her/hers)
Pediatric Hospital Medicine Fellow
Baylor College of Medicine/Texas Children's Hospital
Houston, Texas, United States
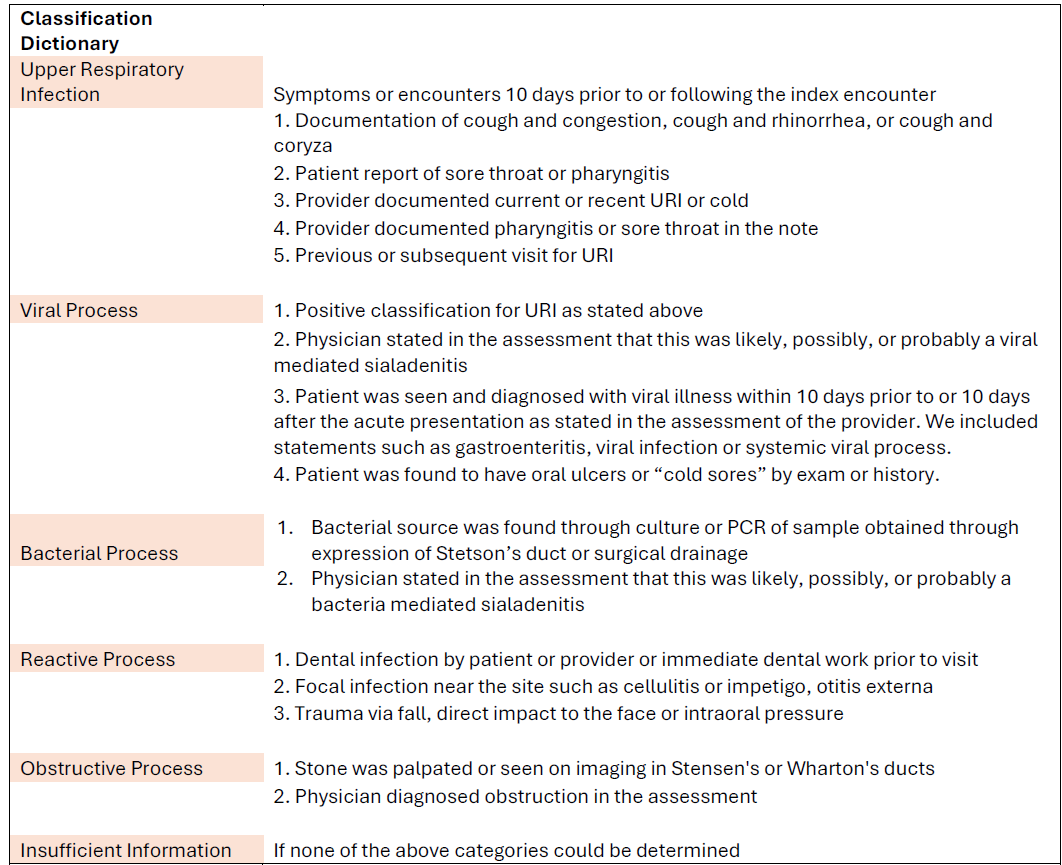 Table 1: Classification Dictionary of Sialadenitis Etiology
Table 1: Classification Dictionary of Sialadenitis Etiology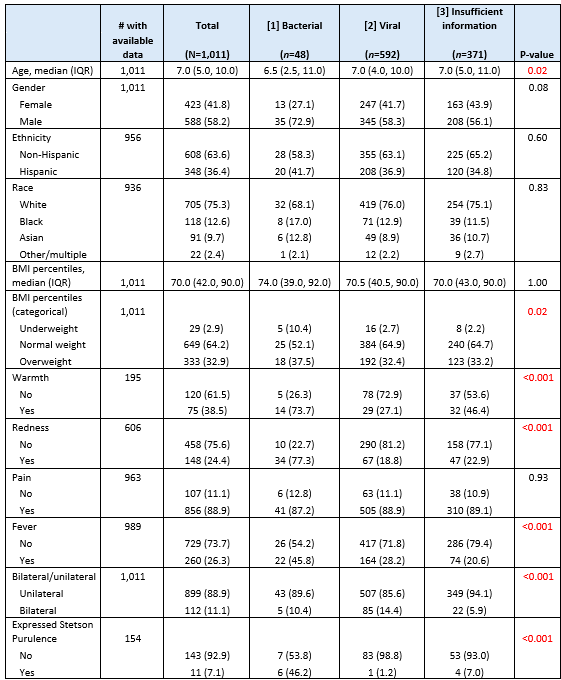 Table 2: Demographic and Presentation Characteristics Separated by Etiology for Patients Aged 0-18 Years Presenting with Sialadenitis
Table 2: Demographic and Presentation Characteristics Separated by Etiology for Patients Aged 0-18 Years Presenting with Sialadenitis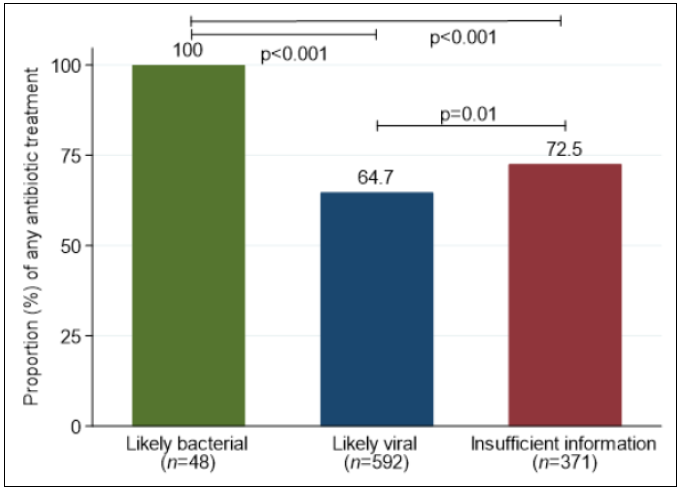 Figure 1: Proportion of Patients Treated with Any Antibiotics Separated by Etiology Classification
Figure 1: Proportion of Patients Treated with Any Antibiotics Separated by Etiology Classification