
Global Neonatal & Children's Health 4
Session: Global Neonatal & Children's Health 4
 photo")
Amy Mackay, MD, MPH (she/her/hers)
Assistant Professor
University of Alabama at Birmingham School of Medicine
Birmingham, Alabama, United States
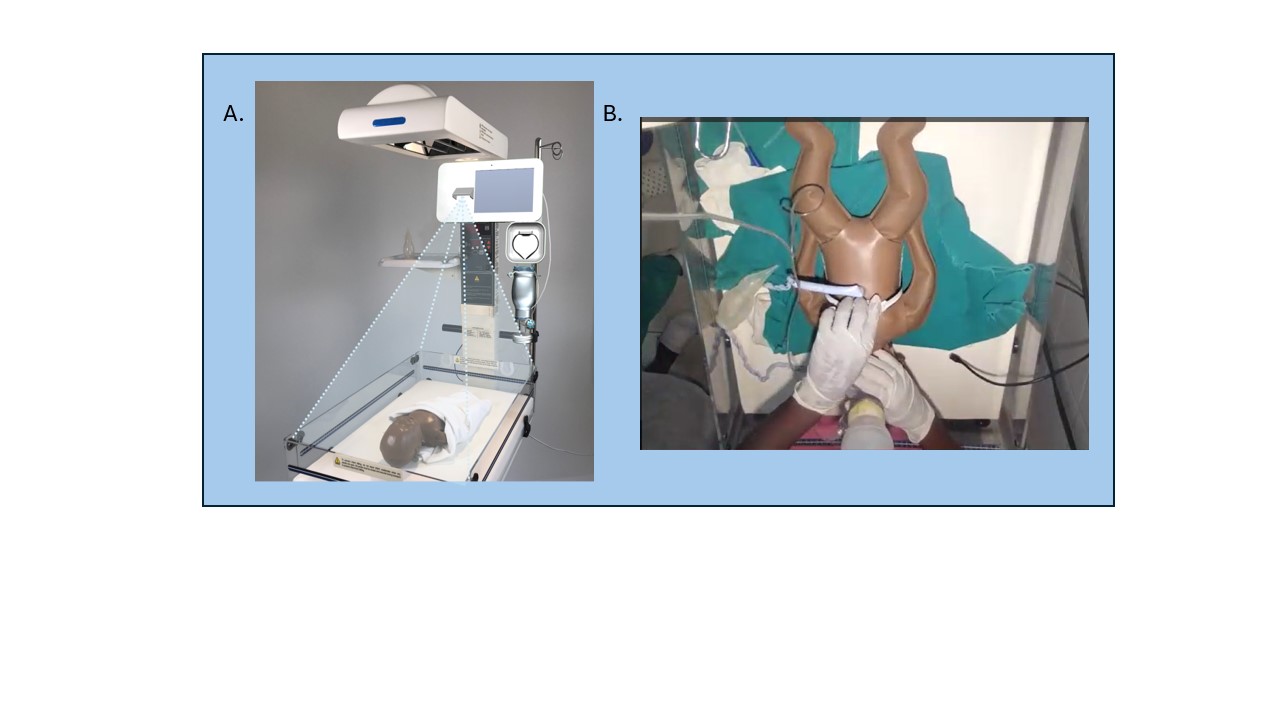 We conducted simulated resuscitations using the Liveborn Station and Neonatalie Live (A). Liveborn Station is a warmer bed with an embedded tablet for video recording, a penguin suction, an upright bag and mask, and NeoBeat (a battery-operated heart rate meter). NeoNatalie Live is a high-fidelity manikin with four programmed scenarios of varying lung compliance. During simulations, the coach connected with the midwife via Zoom (B) to visualize the resuscitation and provide advice.
We conducted simulated resuscitations using the Liveborn Station and Neonatalie Live (A). Liveborn Station is a warmer bed with an embedded tablet for video recording, a penguin suction, an upright bag and mask, and NeoBeat (a battery-operated heart rate meter). NeoNatalie Live is a high-fidelity manikin with four programmed scenarios of varying lung compliance. During simulations, the coach connected with the midwife via Zoom (B) to visualize the resuscitation and provide advice. 
 We conducted simulated resuscitations using the Liveborn Station and Neonatalie Live (A). Liveborn Station is a warmer bed with an embedded tablet for video recording, a penguin suction, an upright bag and mask, and NeoBeat (a battery-operated heart rate meter). NeoNatalie Live is a high-fidelity manikin with four programmed scenarios of varying lung compliance. During simulations, the coach connected with the midwife via Zoom (B) to visualize the resuscitation and provide advice.
We conducted simulated resuscitations using the Liveborn Station and Neonatalie Live (A). Liveborn Station is a warmer bed with an embedded tablet for video recording, a penguin suction, an upright bag and mask, and NeoBeat (a battery-operated heart rate meter). NeoNatalie Live is a high-fidelity manikin with four programmed scenarios of varying lung compliance. During simulations, the coach connected with the midwife via Zoom (B) to visualize the resuscitation and provide advice. 