
Obesity 2
Session: Obesity 2
.jpg "Brittany J. Johnson, BND, BHSc(hons), PhD (she/her/hers) photo")
Brittany J. Johnson, BND, BHSc(hons), PhD (she/her/hers)
Senior Research Fellow
Flinders University
Bedford Park, South Australia, Australia
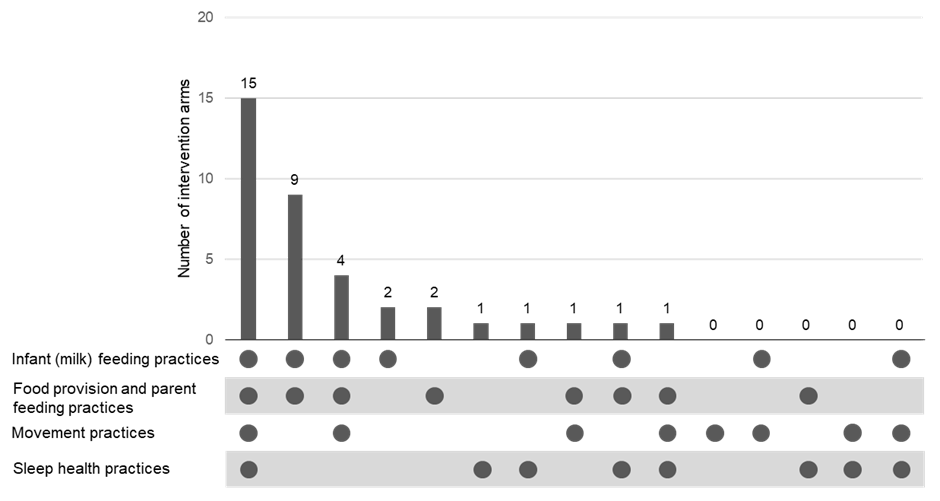 a The x-axis details the possible combinations of the four target parental behaviour clusters, with the dots indicating cluster present in that combination. The y-axis indicates the number of interventions that targeted that combination of clusters. Zeros represent that no intervention targeted the combination of clusters.
a The x-axis details the possible combinations of the four target parental behaviour clusters, with the dots indicating cluster present in that combination. The y-axis indicates the number of interventions that targeted that combination of clusters. Zeros represent that no intervention targeted the combination of clusters.