
General Pediatrics 4
Session: General Pediatrics 4

Hannah K. Bassett, MD
Clinical Associate Professor
Stanford University School of Medicine
Redwood City, California, United States
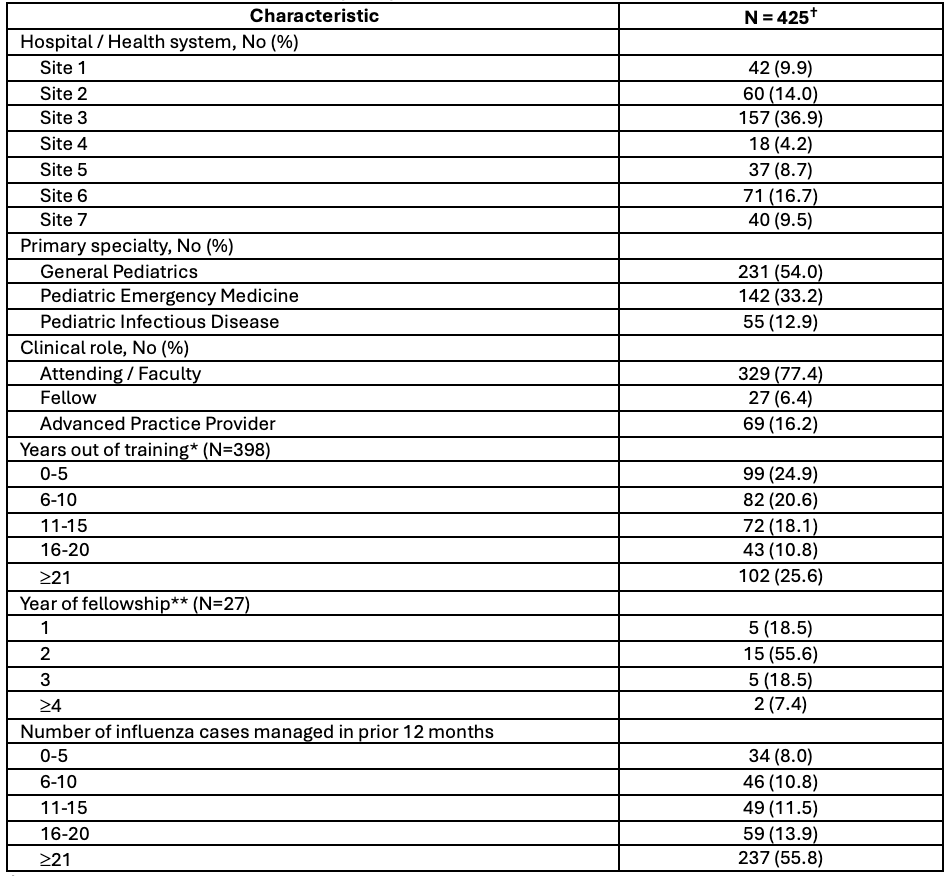 †Numbers for demographic groups may not add up to 425 as not all respondents completed all questions of the survey
†Numbers for demographic groups may not add up to 425 as not all respondents completed all questions of the survey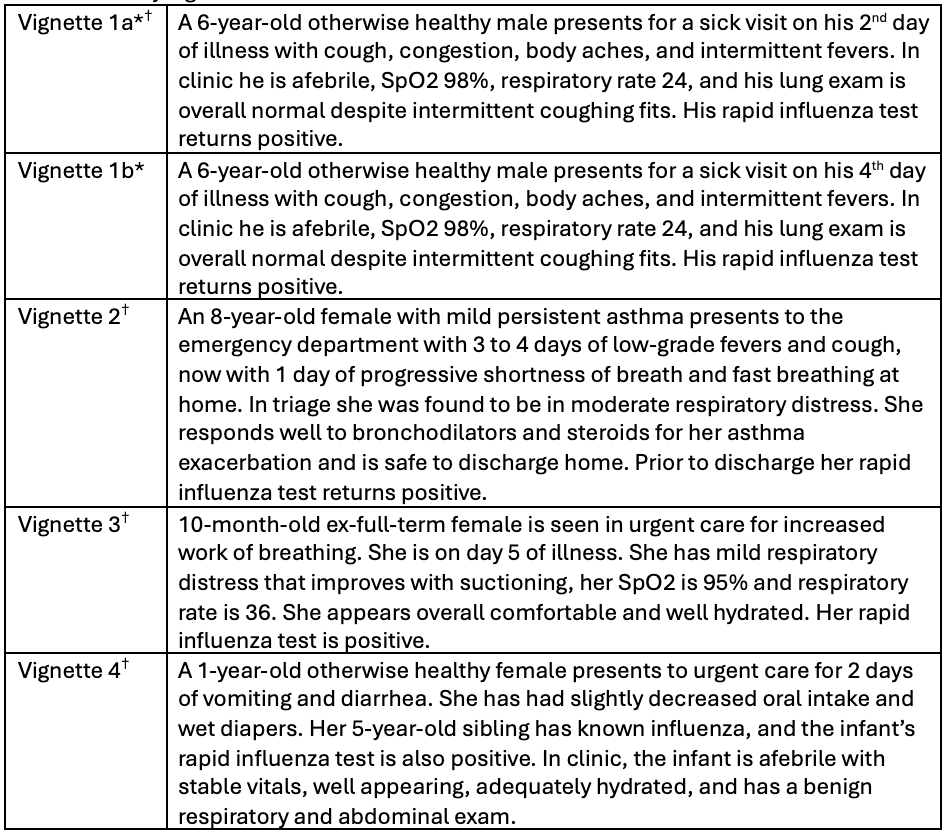 *Vignette 1 was randomized amongst respondents 50:50 into 1a and 1b.
*Vignette 1 was randomized amongst respondents 50:50 into 1a and 1b.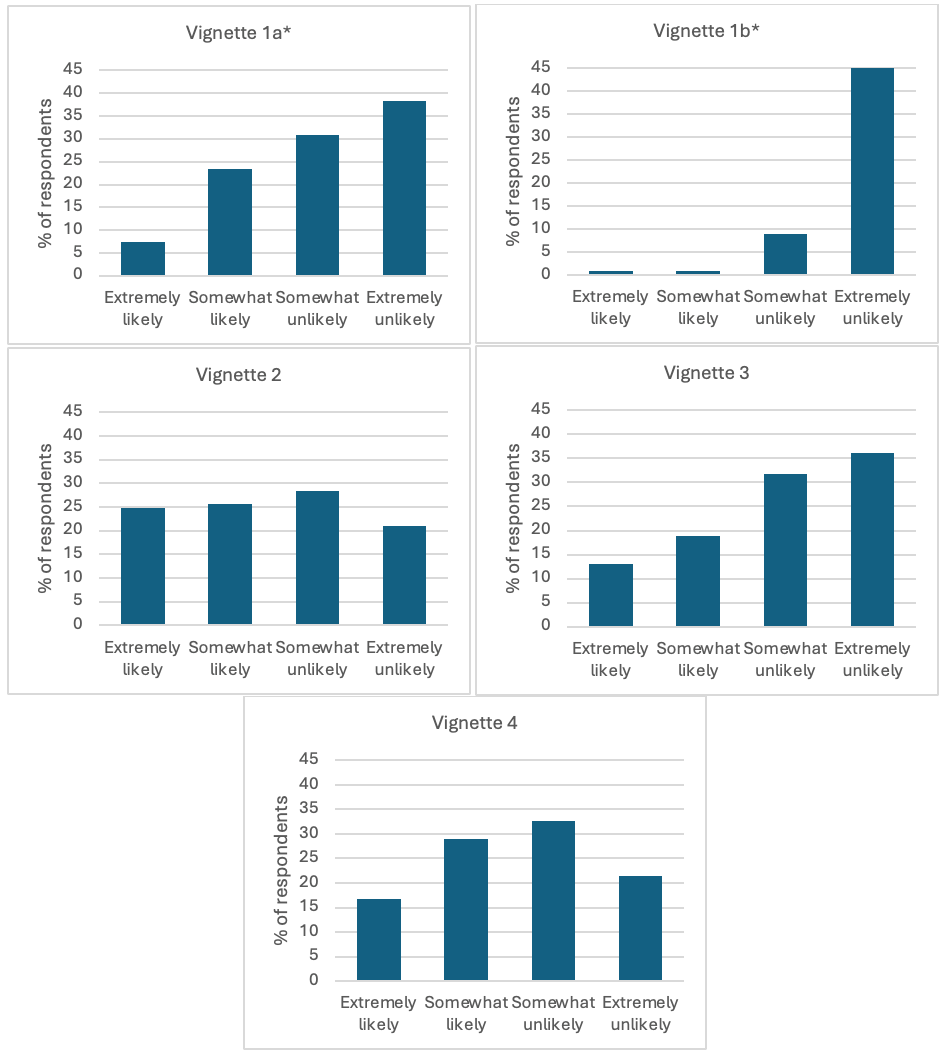 Unadjusted likelihood to recommend oseltamivir for each clinical vignette. *Significant difference (p < 0.001) in likelihood to recommend oseltamivir between the randomized version of vignette 1 (a vs b).
Unadjusted likelihood to recommend oseltamivir for each clinical vignette. *Significant difference (p < 0.001) in likelihood to recommend oseltamivir between the randomized version of vignette 1 (a vs b).