
Emergency Medicine 8
Session: Emergency Medicine 8
 Credit")

Greg Stewart, MD
Associate Professor of Pediatric Emergency Medicine
Nationwide Childrens Hospital
Columbus, Ohio, United States
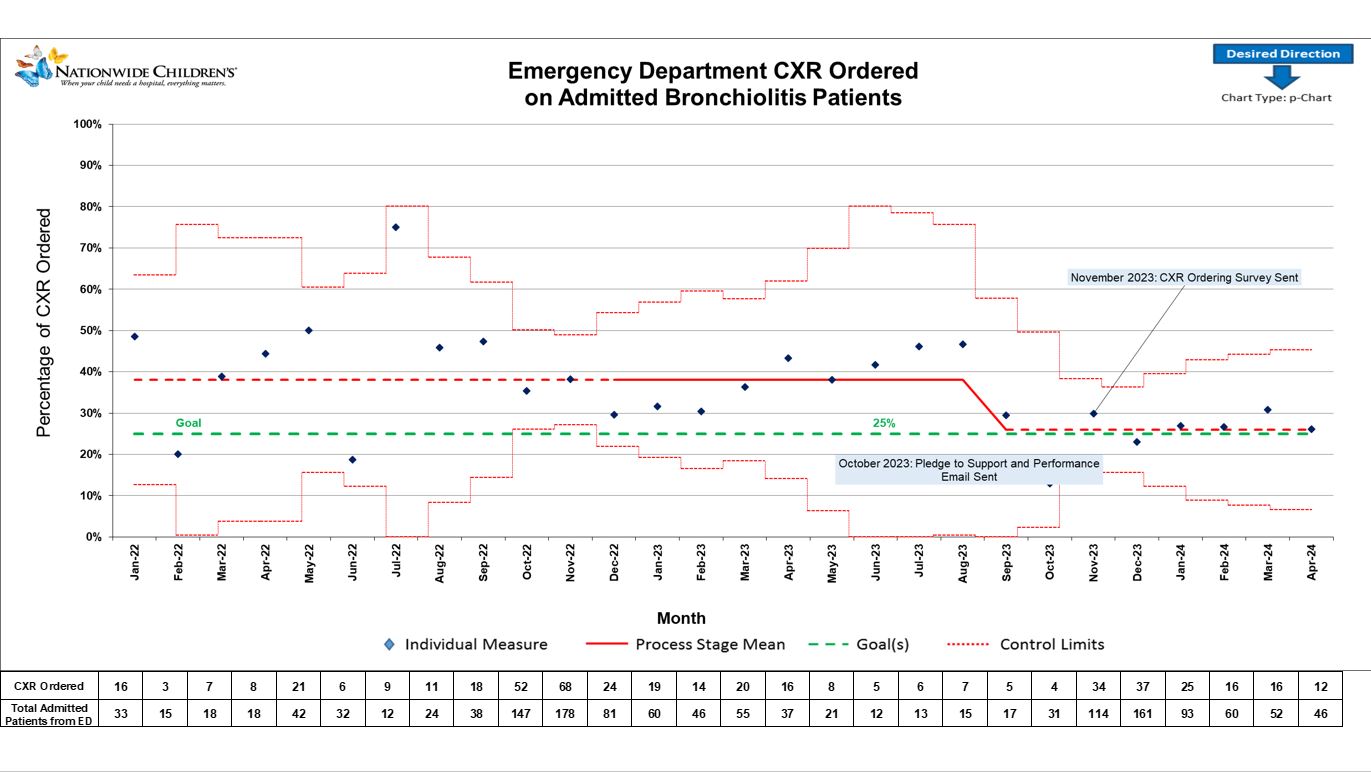 Emergency Department adaption of ROUTT-B strategies and department specific strategies reduced the rate of CXR in the ED from 38% to 26%.
Emergency Department adaption of ROUTT-B strategies and department specific strategies reduced the rate of CXR in the ED from 38% to 26%. This Pledge to Support was signed by Hospital Pediatrics and Infectious Diseases Faculty stating they support the ED in following the AAP guidelines regarding Chest X-Rays in patients with the primary diagnosis of bronchiolitis. ED decrease in CXR ordering did not lead to a supplemental increase in inpatient CXR ordering.
This Pledge to Support was signed by Hospital Pediatrics and Infectious Diseases Faculty stating they support the ED in following the AAP guidelines regarding Chest X-Rays in patients with the primary diagnosis of bronchiolitis. ED decrease in CXR ordering did not lead to a supplemental increase in inpatient CXR ordering..jpg) After implementation of an ED QI project to adapt ROUTT-B strategies, a decrease of CXR ordering for bronchiolitis was seen from 37% baseline to 29%.
After implementation of an ED QI project to adapt ROUTT-B strategies, a decrease of CXR ordering for bronchiolitis was seen from 37% baseline to 29%.