
Global Neonatal & Children's Health 3
Session: Global Neonatal & Children's Health 3

Alvaro Proaño, MD
Neonatal-Perinatal Medicine Fellow
Childrens Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
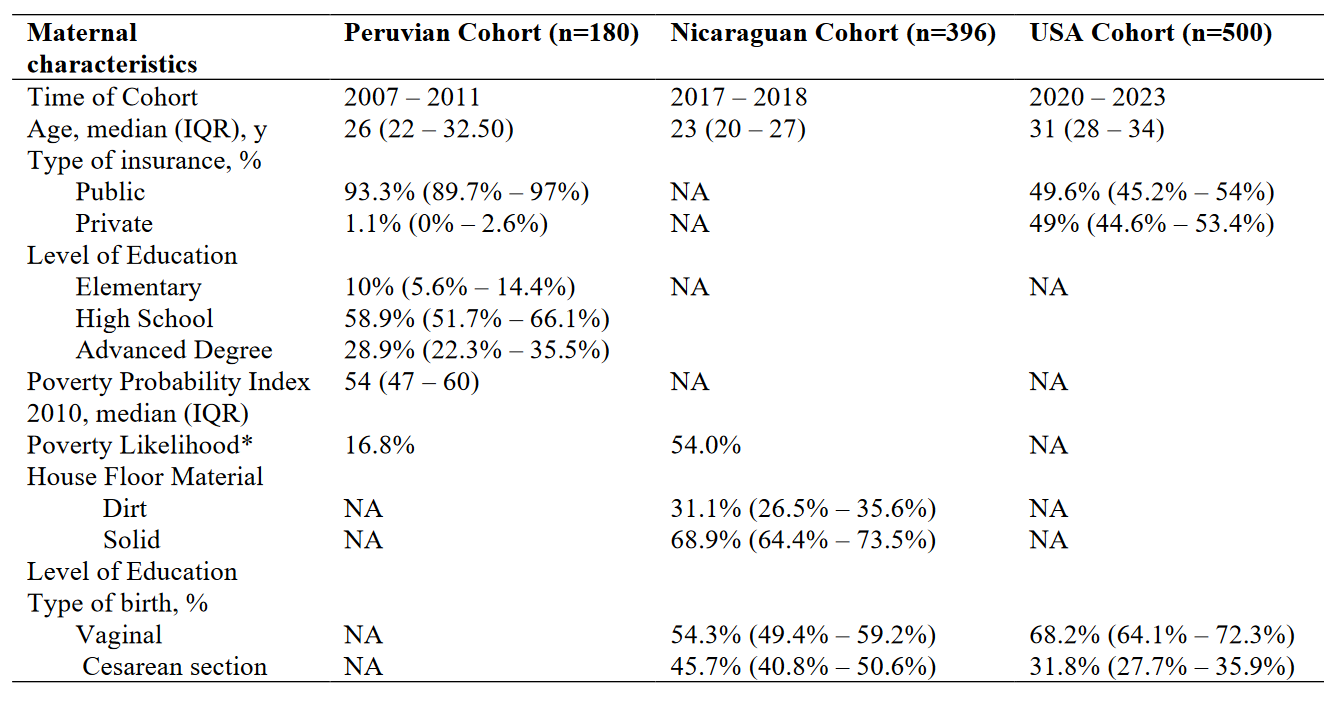 *Poverty likelihood was calculated differently for Peruvian and Nicaraguan Cohorts, the Peruvian Cohort utilized the Poverty Probability Index published in Ballard SB, Requena D, Mayta H, Sanchez GJ, Oyola-Lozada MG, Colquechagua Aliaga FD, Cabrera L, Vittet Mondonedo MD, Taquiri C, Tilley CDH, Simons CMP, Meza RA, Bern C, Saito M, Figueroa-Quintanilla DA, Gilman RH. Enteropathogen Changes After Rotavirus Vaccine Scale-up. Pediatrics. 2022 Jan 1;149(1):e2020049884. doi: 10.1542/peds.2020-049884. PMID: 34918158; PMCID: PMC9647525, while the Nicaraguan Cohort used the Poverty Index published in Vielot NA, González F, Reyes Y, Zepeda O, Blette B, Paniagua M, Toval-Ruíz C, Diez-Valcarce M, Hudgens MG, Gutiérrez L, Blandón P, Herrera R, Cuadra EC, Bowman N, Vilchez S, Vinjé J, Becker-Dreps S, Bucardo F. Risk Factors and Clinical Profile of Sapovirus-associated Acute Gastroenteritis in Early Childhood: A Nicaraguan Birth Cohort Study. Pediatr Infect Dis J. 2021 Mar 1;40(3):220-226. doi: 10.1097/INF.0000000000003015. PMID: 33464013; PMCID: PMC7878336.
*Poverty likelihood was calculated differently for Peruvian and Nicaraguan Cohorts, the Peruvian Cohort utilized the Poverty Probability Index published in Ballard SB, Requena D, Mayta H, Sanchez GJ, Oyola-Lozada MG, Colquechagua Aliaga FD, Cabrera L, Vittet Mondonedo MD, Taquiri C, Tilley CDH, Simons CMP, Meza RA, Bern C, Saito M, Figueroa-Quintanilla DA, Gilman RH. Enteropathogen Changes After Rotavirus Vaccine Scale-up. Pediatrics. 2022 Jan 1;149(1):e2020049884. doi: 10.1542/peds.2020-049884. PMID: 34918158; PMCID: PMC9647525, while the Nicaraguan Cohort used the Poverty Index published in Vielot NA, González F, Reyes Y, Zepeda O, Blette B, Paniagua M, Toval-Ruíz C, Diez-Valcarce M, Hudgens MG, Gutiérrez L, Blandón P, Herrera R, Cuadra EC, Bowman N, Vilchez S, Vinjé J, Becker-Dreps S, Bucardo F. Risk Factors and Clinical Profile of Sapovirus-associated Acute Gastroenteritis in Early Childhood: A Nicaraguan Birth Cohort Study. Pediatr Infect Dis J. 2021 Mar 1;40(3):220-226. doi: 10.1097/INF.0000000000003015. PMID: 33464013; PMCID: PMC7878336. 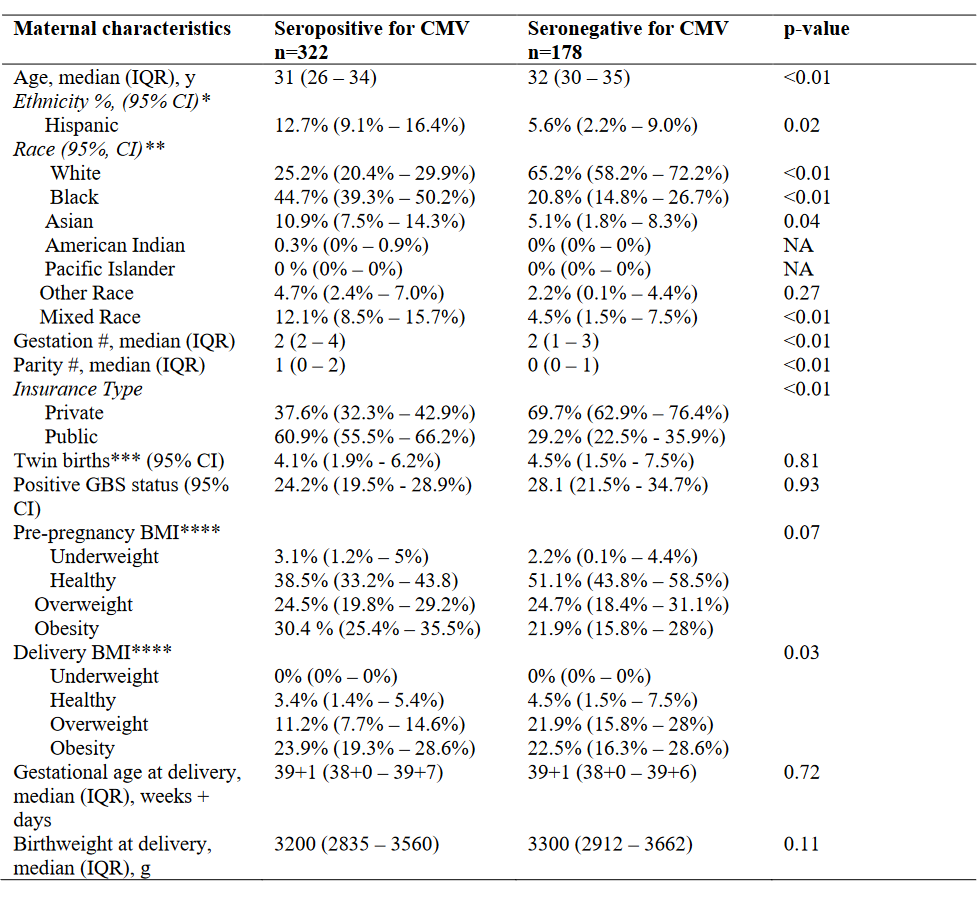 * From the available 500 records, 414 had ethnicity registered. ** From the available 500 records, 489 had race registered. ****Definition per CDC categories.
* From the available 500 records, 414 had ethnicity registered. ** From the available 500 records, 489 had race registered. ****Definition per CDC categories.