
Nephrology 1
Session: Nephrology 1
 photo")
Travis Churilla, MD (he/him/his)
Pediatric Nephrology Fellow, PGY-4
Ann & Robert H. Lurie Children's Hospital of Chicago
Chicago, Illinois, United States
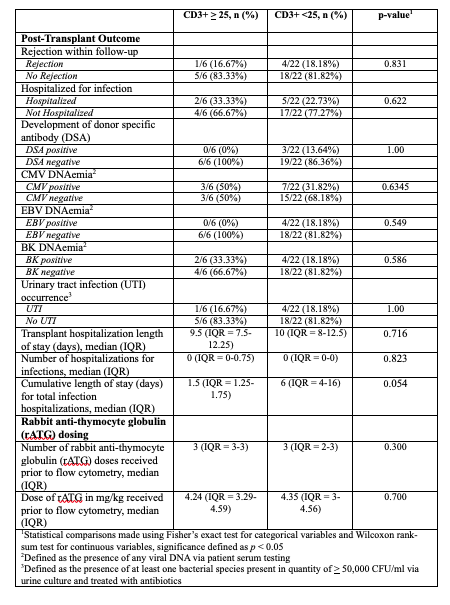 1Statistical comparisons made using Fisher’s exact test for categorical variables and Wilcoxon rank-sum test for continuous variables, significance defined as p < 0.05
1Statistical comparisons made using Fisher’s exact test for categorical variables and Wilcoxon rank-sum test for continuous variables, significance defined as p < 0.05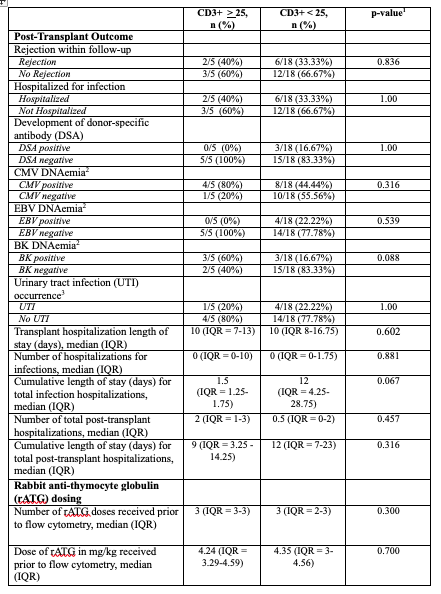 1Statistical comparisons made using Fisher’s exact test for categorical variables and Wilcoxon rank-sum test for continuous variables, significant defined as p < 0.05
1Statistical comparisons made using Fisher’s exact test for categorical variables and Wilcoxon rank-sum test for continuous variables, significant defined as p < 0.05