
Nephrology 6
Session: Nephrology 6
Hailey Connolly, MD (she/her/hers)
Resident Physician
Joseph M. Sanzari Children's Hospital Hackensack University Medical Center
Jersey City, New Jersey, United States
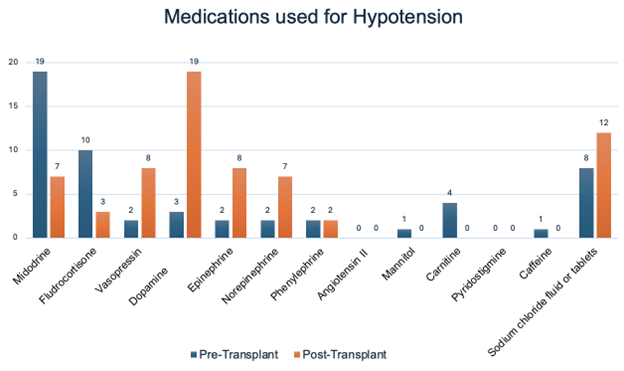 Respondents were asked to select all medications that they used in their practice. In the pre-transplant phase, Midodrine and Fludrocortisone were the most commonly used therapies, with 19 and 10 respondents respectively, while dopamine and vasopressin were less frequently utilized. Post-transplant, dopamine and epinephrine emerged as the most used therapies with 19 and 8 respondents respectively, indicating a shift in medication preferences following the transplant.Respondents were asked to select all medications that they used in their practice. In the pre-transplant phase, Midodrine and Fludrocortisone were the most commonly used therapies, with 19 and 10 respondents respectively, while dopamine and vasopressin were less frequently utilized. Post-transplant, dopamine and epinephrine emerged as the most used therapies with 19 and 8 respondents respectively, indicating a shift in medication preferences following the transplant.
Respondents were asked to select all medications that they used in their practice. In the pre-transplant phase, Midodrine and Fludrocortisone were the most commonly used therapies, with 19 and 10 respondents respectively, while dopamine and vasopressin were less frequently utilized. Post-transplant, dopamine and epinephrine emerged as the most used therapies with 19 and 8 respondents respectively, indicating a shift in medication preferences following the transplant.Respondents were asked to select all medications that they used in their practice. In the pre-transplant phase, Midodrine and Fludrocortisone were the most commonly used therapies, with 19 and 10 respondents respectively, while dopamine and vasopressin were less frequently utilized. Post-transplant, dopamine and epinephrine emerged as the most used therapies with 19 and 8 respondents respectively, indicating a shift in medication preferences following the transplant.