
Nephrology 4
Session: Nephrology 4
 photo")
Daniel S. Thomson, MD (he/him/his)
Pediatric Resident
University of Colorado School of Medicine
Denver, Colorado, United States
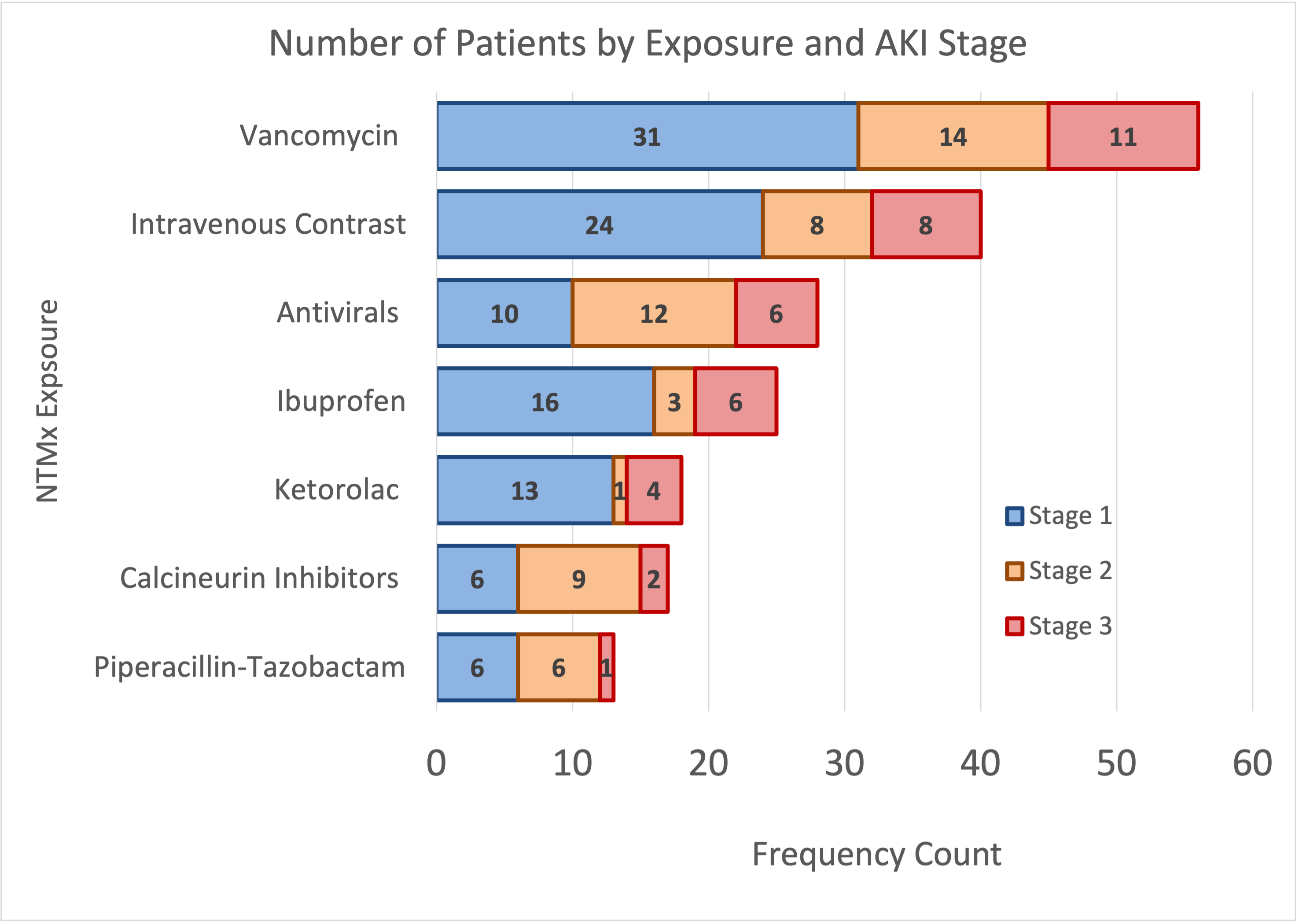 All NTMx exposures are grouped, showing total number of patients that were exposed to that specific medication group and patient AKI stage. Calcineurin inhibitors include tacrolimus and cyclosporine, antiviral medications include acyclovir, ganciclovir, valganciclovir, and valacyclovir.
All NTMx exposures are grouped, showing total number of patients that were exposed to that specific medication group and patient AKI stage. Calcineurin inhibitors include tacrolimus and cyclosporine, antiviral medications include acyclovir, ganciclovir, valganciclovir, and valacyclovir.