
Emergency Medicine 8
Session: Emergency Medicine 8
Peter Dayan, MD, MSc (he/him/his)
Director of Research, Pediatric Emergency Medicine
Columbia University
Hastings on Hudson, New York, United States
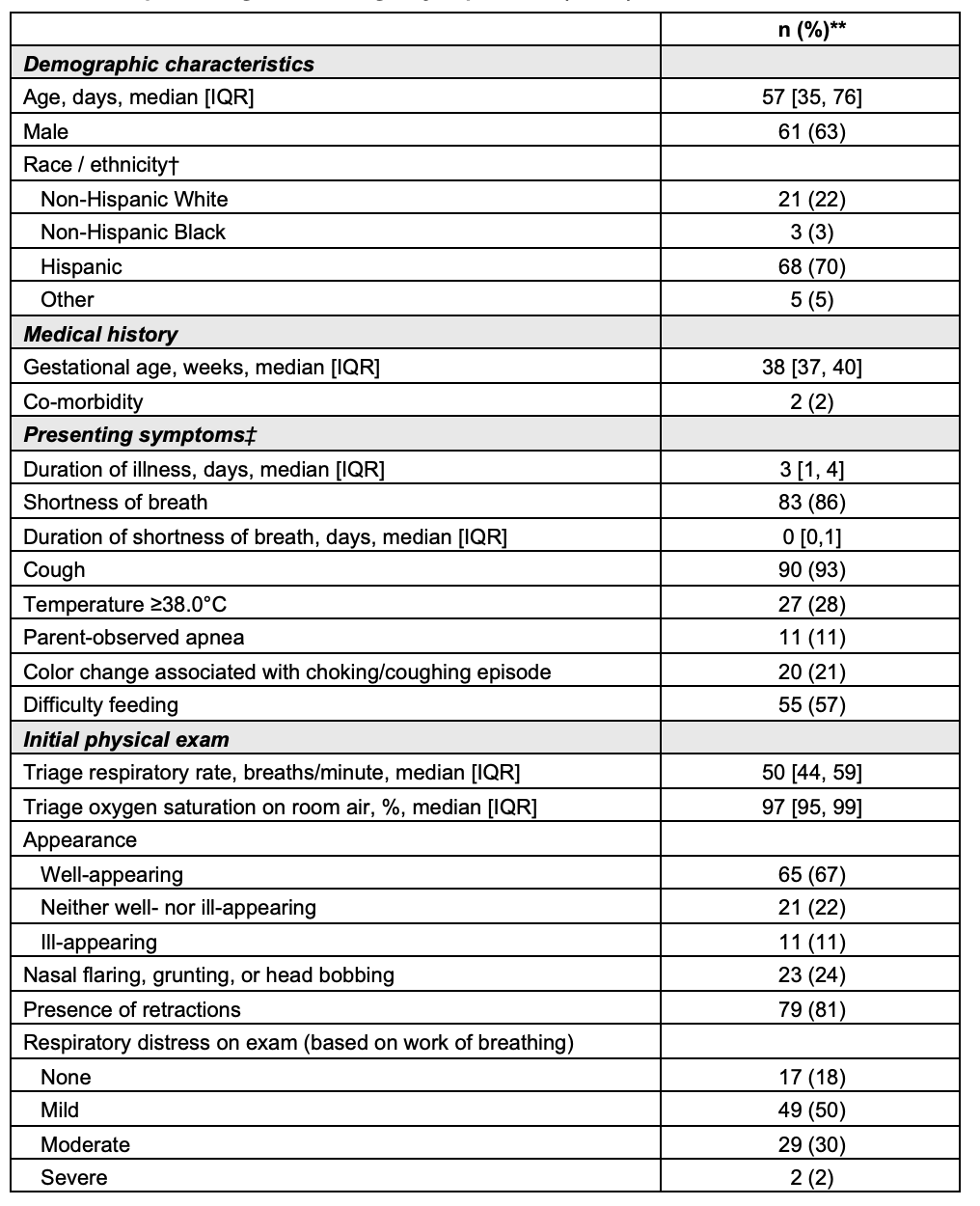 * Total number includes infants who had at least 15 minutes of continuously measured oxygen saturation data.
* Total number includes infants who had at least 15 minutes of continuously measured oxygen saturation data. .png) * Oxygen saturation thresholds were selected based on available bronchiolitis guidelines from USA (AAP, 2014: ≤90%), UK (NICE, 2015: ≤91%), Italy (2014: ≤89-91%), Spain (2010: ≤91%), and France (2013: ≤91%).
* Oxygen saturation thresholds were selected based on available bronchiolitis guidelines from USA (AAP, 2014: ≤90%), UK (NICE, 2015: ≤91%), Italy (2014: ≤89-91%), Spain (2010: ≤91%), and France (2013: ≤91%).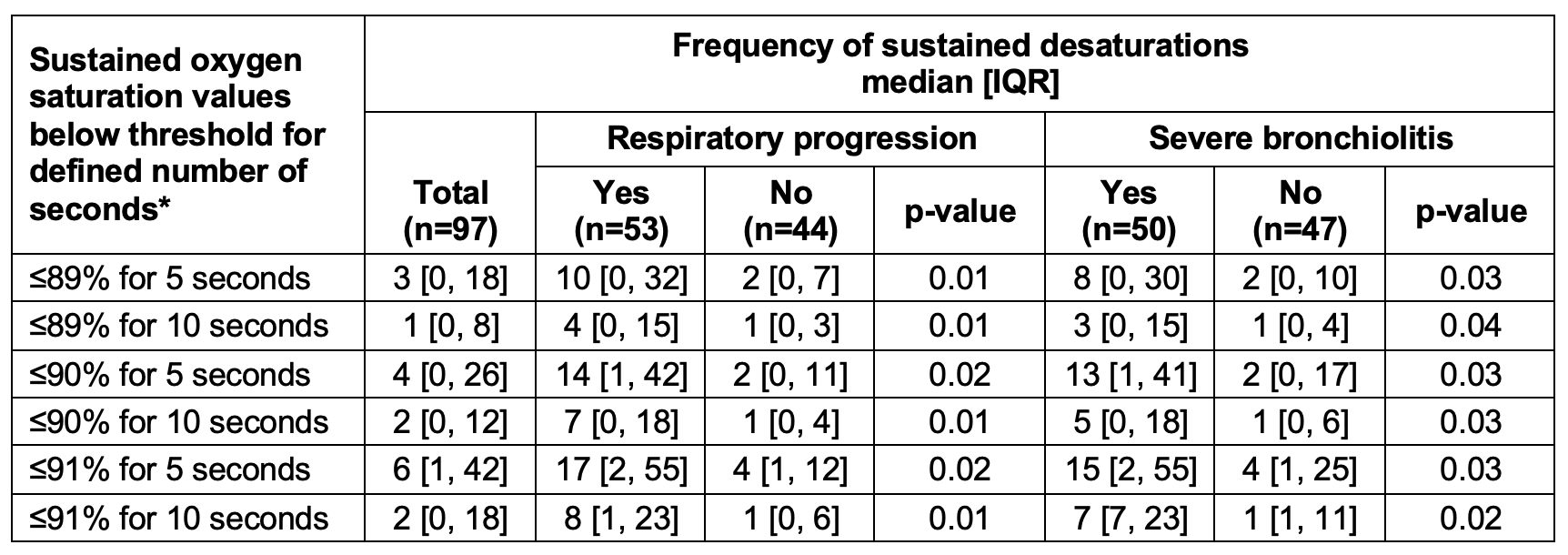 * Sustained desaturation was defined as consecutive desaturations lasting five or ten seconds. These consecutive desaturations were selected to capture true desaturations, minimizing the likelihood of artifacts or measurement errors. To account for differences in the duration of SpO2 data available for each patient, frequency of sustained desaturations was normalized. * Total number includes infants who had at least 15 minutes of continuously measured oxygen saturation data. * Oxygen saturation thresholds were selected based on available bronchiolitis guidelines from USA (AAP, 2014: ≤90%), UK (NICE, 2015: ≤91%), Italy (2014: ≤89-91%), Spain (2010: ≤91%), and France (2013: ≤91%).* Sustained desaturation was defined as consecutive desaturations lasting five or ten seconds. These consecutive desaturations were selected to capture true desaturations, minimizing the likelihood of artifacts or measurement errors. To account for differences in the duration of SpO2 data available for each patient, frequency of sustained desaturations was normalized.
* Sustained desaturation was defined as consecutive desaturations lasting five or ten seconds. These consecutive desaturations were selected to capture true desaturations, minimizing the likelihood of artifacts or measurement errors. To account for differences in the duration of SpO2 data available for each patient, frequency of sustained desaturations was normalized. * Total number includes infants who had at least 15 minutes of continuously measured oxygen saturation data. * Oxygen saturation thresholds were selected based on available bronchiolitis guidelines from USA (AAP, 2014: ≤90%), UK (NICE, 2015: ≤91%), Italy (2014: ≤89-91%), Spain (2010: ≤91%), and France (2013: ≤91%).* Sustained desaturation was defined as consecutive desaturations lasting five or ten seconds. These consecutive desaturations were selected to capture true desaturations, minimizing the likelihood of artifacts or measurement errors. To account for differences in the duration of SpO2 data available for each patient, frequency of sustained desaturations was normalized. 