
Global Neonatal & Children's Health 4
Session: Global Neonatal & Children's Health 4
 photo")
Sahar T. Rahiem, MD, MHS (she/her/hers)
Perinatal-Neonatal Fellow
University of Washington School of Medicine
Seattle, Washington, United States
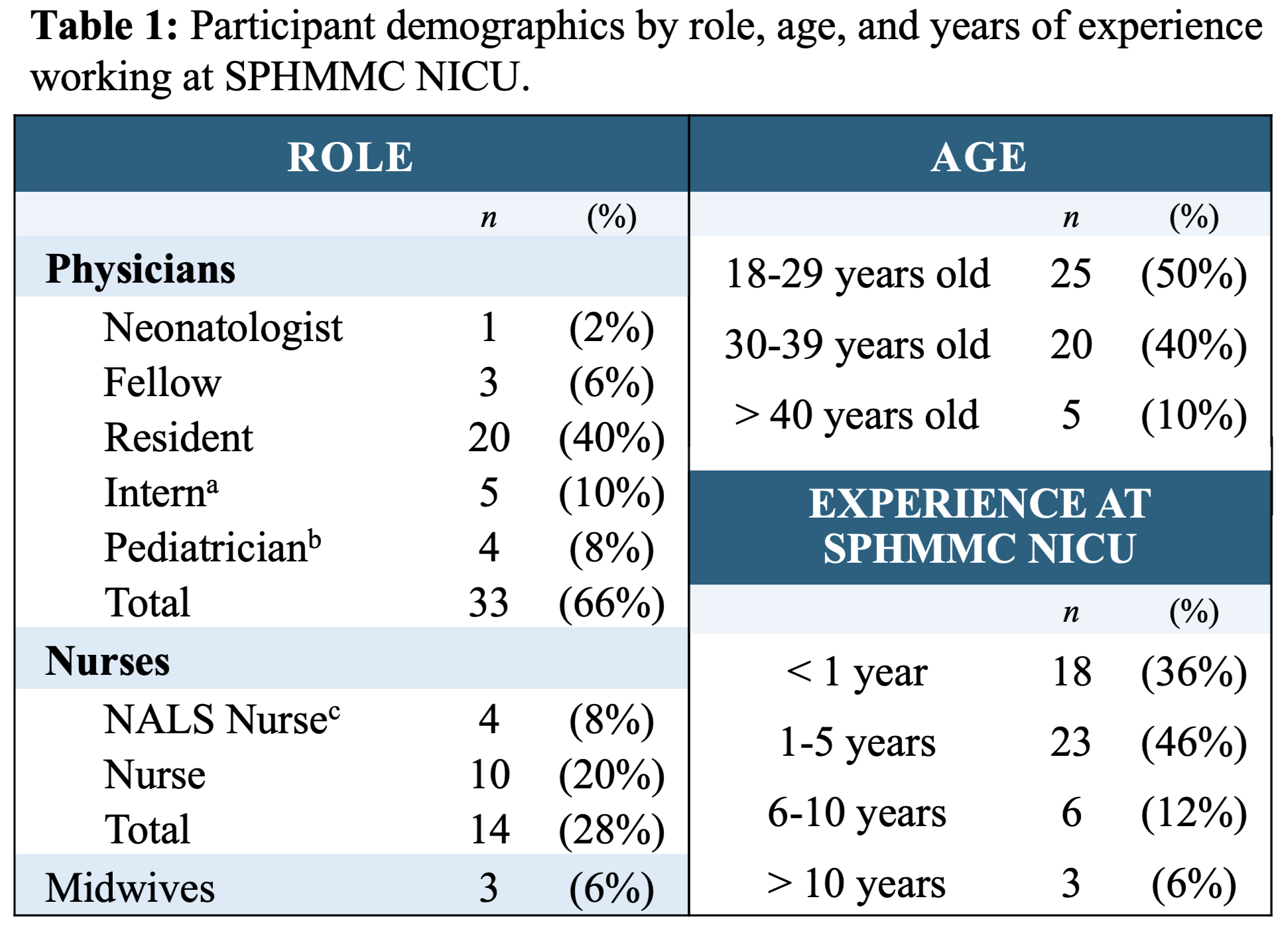 a An intern is in their final year of medical school and considered a physician in Ethiopia.
a An intern is in their final year of medical school and considered a physician in Ethiopia.
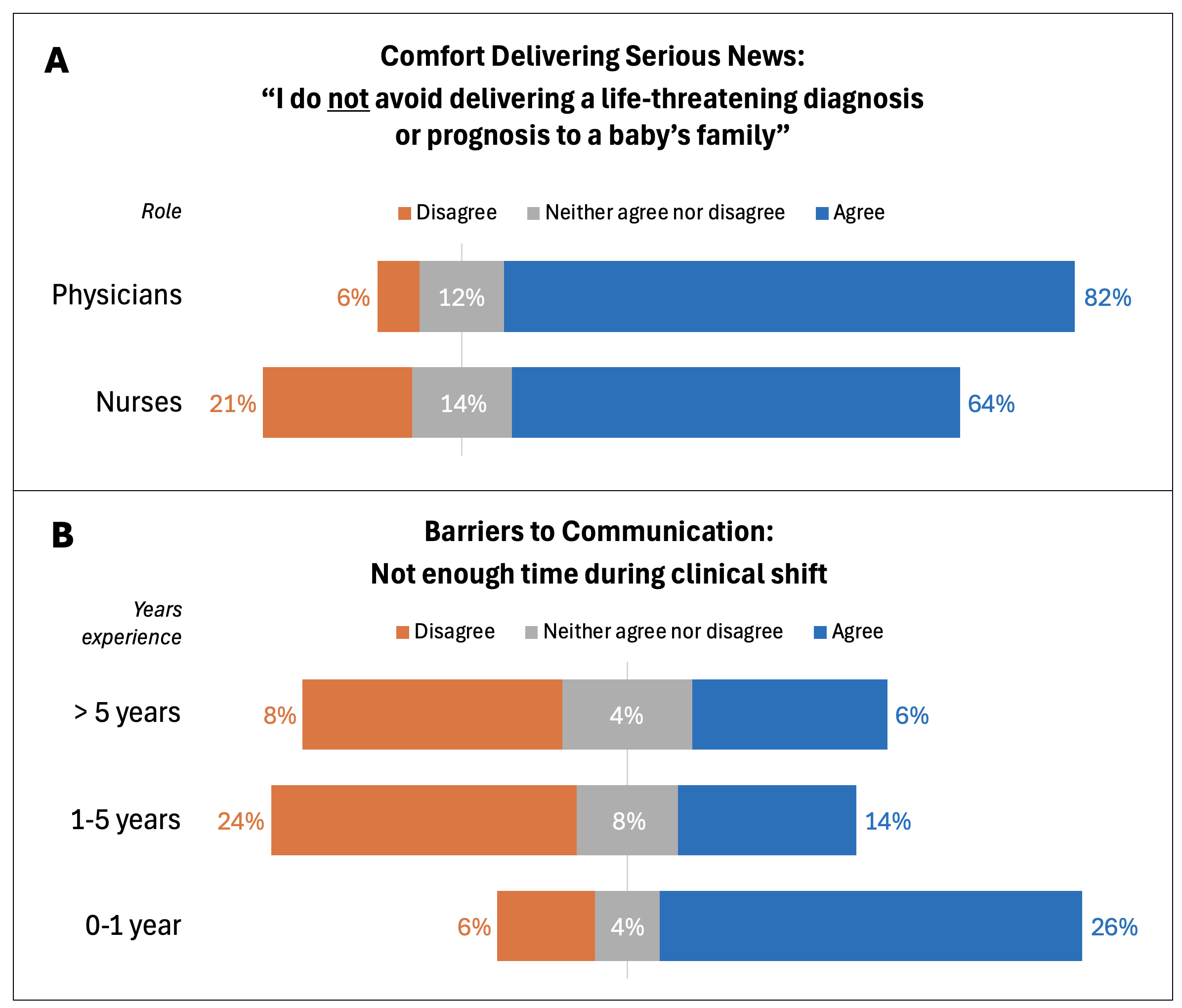 2A: Physicians in the NICU report less avoidance delivering serious news to patient families than nurses. 2B: “Not enough time during a clinical shift” as a barrier to communication with patient families correlated to years of work experience. Healthcare providers with more than 5 years of experience do not report having enough time during their clinical shift as a barrier to communicating with patient families as much as providers with fewer years experience.a An intern is in their final year of medical school and considered a physician in Ethiopia.2A: Physicians in the NICU report less avoidance delivering serious news to patient families than nurses. 2B: “Not enough time during a clinical shift” as a barrier to communication with patient families correlated to years of work experience. Healthcare providers with more than 5 years of experience do not report having enough time during their clinical shift as a barrier to communicating with patient families as much as providers with fewer years experience.
2A: Physicians in the NICU report less avoidance delivering serious news to patient families than nurses. 2B: “Not enough time during a clinical shift” as a barrier to communication with patient families correlated to years of work experience. Healthcare providers with more than 5 years of experience do not report having enough time during their clinical shift as a barrier to communicating with patient families as much as providers with fewer years experience.a An intern is in their final year of medical school and considered a physician in Ethiopia.2A: Physicians in the NICU report less avoidance delivering serious news to patient families than nurses. 2B: “Not enough time during a clinical shift” as a barrier to communication with patient families correlated to years of work experience. Healthcare providers with more than 5 years of experience do not report having enough time during their clinical shift as a barrier to communicating with patient families as much as providers with fewer years experience.