
General Pediatrics 3
Session: General Pediatrics 3
 photo")
Rashedat Oshodi, MD (she/her/hers)
Pediatric Physician
University of Minnesota Medical School
Eden Prairie, Minnesota, United States
.png)
 The reference group is US-born parents.
The reference group is US-born parents.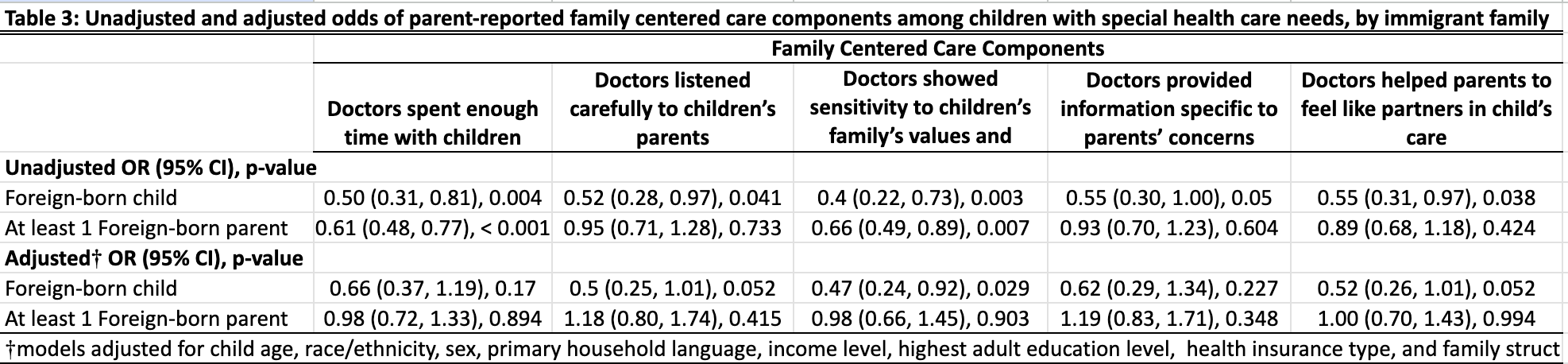 The reference group is US-born parents.The reference group is US-born parents.The reference group is US-born parents.
The reference group is US-born parents.The reference group is US-born parents.The reference group is US-born parents.