
Emergency Medicine 7
Session: Emergency Medicine 7
 photo")
Hannah Sneller, MD (she/her/hers)
Pediatric Emergency Physician/Associate Professor of Pediatrics
Children's Nebraska
Omaha, Nebraska, United States
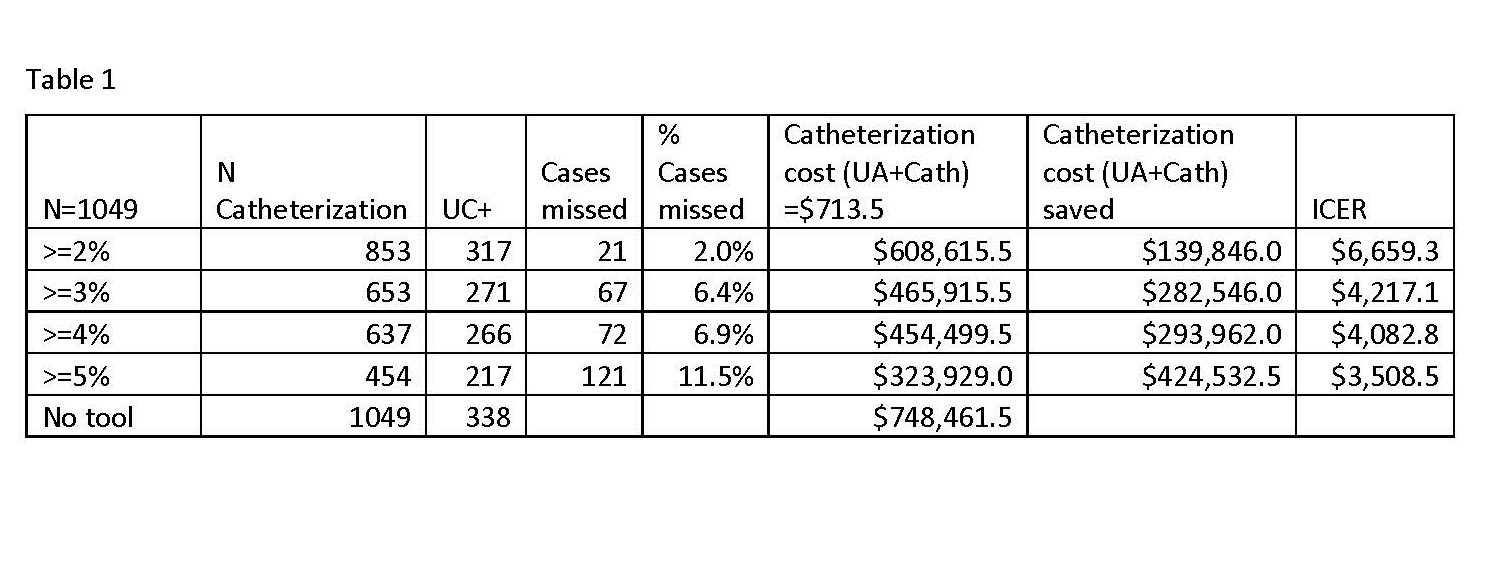 Cases missed, cost savings, and ICER for different cutoff points , using unit catheterization cost of $713.50.
Cases missed, cost savings, and ICER for different cutoff points , using unit catheterization cost of $713.50.