
Hospital Medicine 5: Clinical
Session: Hospital Medicine 5: Clinical
Jennifer T. Stamp, MD (she/her/hers)
Resident
Phoenix Children's Hospital
Phoenix, Arizona, United States
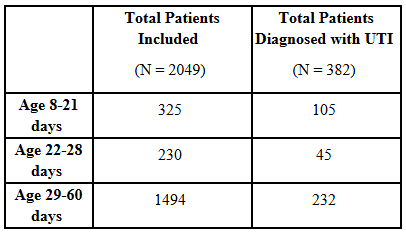 Table 1: Study Demographics
Table 1: Study Demographics.png) Table 2: Comparison of Urinalysis Component Sensitivity Between 8-21, 22-28, and 29-60 Day Old Febrile Infants
Table 2: Comparison of Urinalysis Component Sensitivity Between 8-21, 22-28, and 29-60 Day Old Febrile Infants .png) Table 3: Comparison of Urinalysis Component Specificity Between 8-21, 22-28, and 29-60 Day Old Febrile Infants
Table 3: Comparison of Urinalysis Component Specificity Between 8-21, 22-28, and 29-60 Day Old Febrile Infants 