
Neonatal Quality Improvement 5
Session: Neonatal Quality Improvement 5
 Credit")
 photo")
somaya abuelazm, MD,FAAP (she/her/hers)
NPM fellow
Cleveland Clinic Children's
Cleveland, Ohio, United States
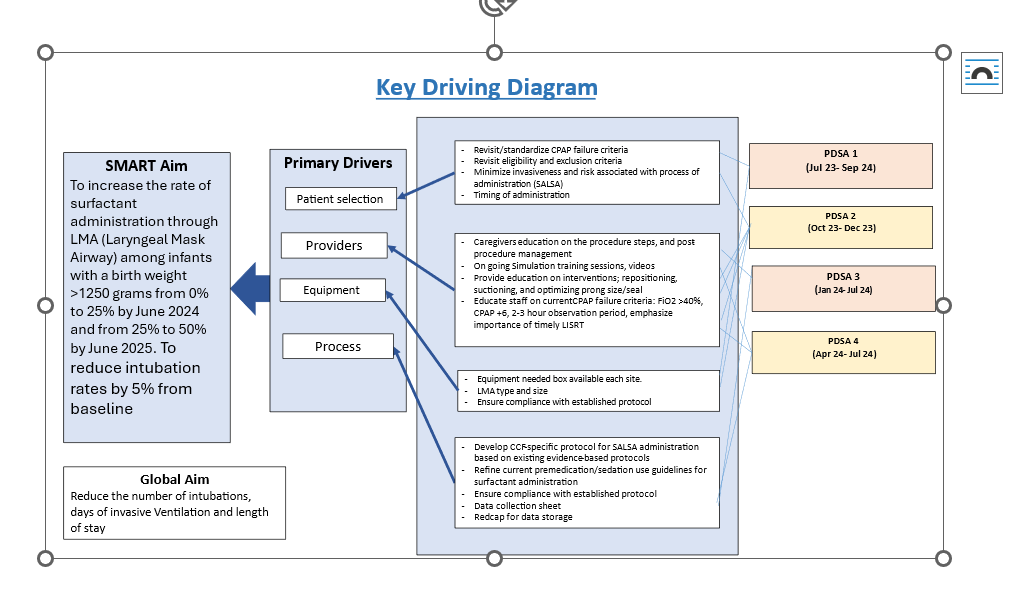 key driver diagram
key driver diagram 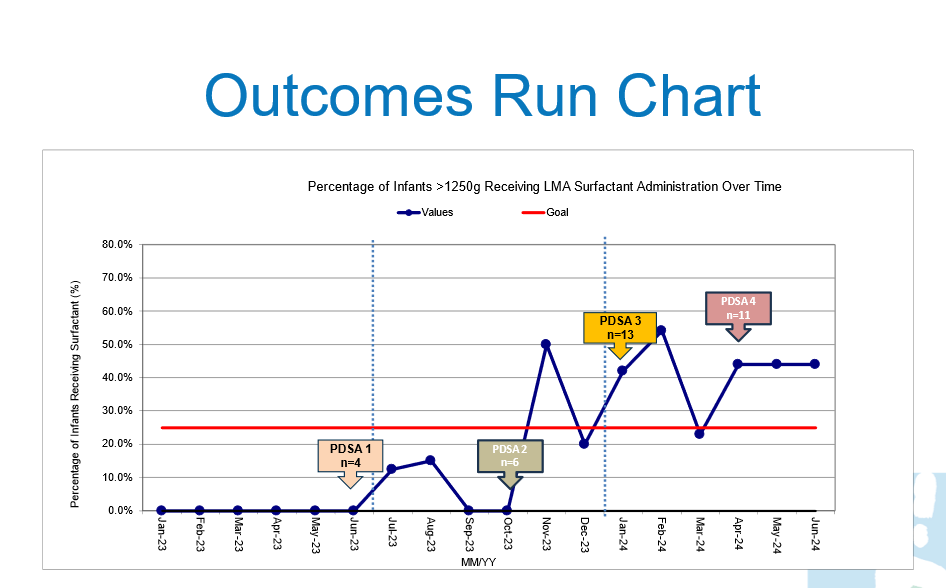 outcome Run Chart, surfactant administration rates via laryngeal mask airway
outcome Run Chart, surfactant administration rates via laryngeal mask airway 