
Neonatal Quality Improvement 6
Session: Neonatal Quality Improvement 6
 Credit")
Chelsey A. Bithell, MD (she/her/hers)
Fellow
MedStar Georgetown University Hospital
Chevy Chase, Maryland, United States
.jpg) PPD screening completion rate between November 19th and October 6th. Interventions noted in red boxes. Total percentage of screens completed has improved from about 25% at the start of the study to 56% over a period of one year.
PPD screening completion rate between November 19th and October 6th. Interventions noted in red boxes. Total percentage of screens completed has improved from about 25% at the start of the study to 56% over a period of one year..jpg) PPD screening completion rate for mothers and fathers. Compliance for fathers is generally lower than for mothers.
PPD screening completion rate for mothers and fathers. Compliance for fathers is generally lower than for mothers.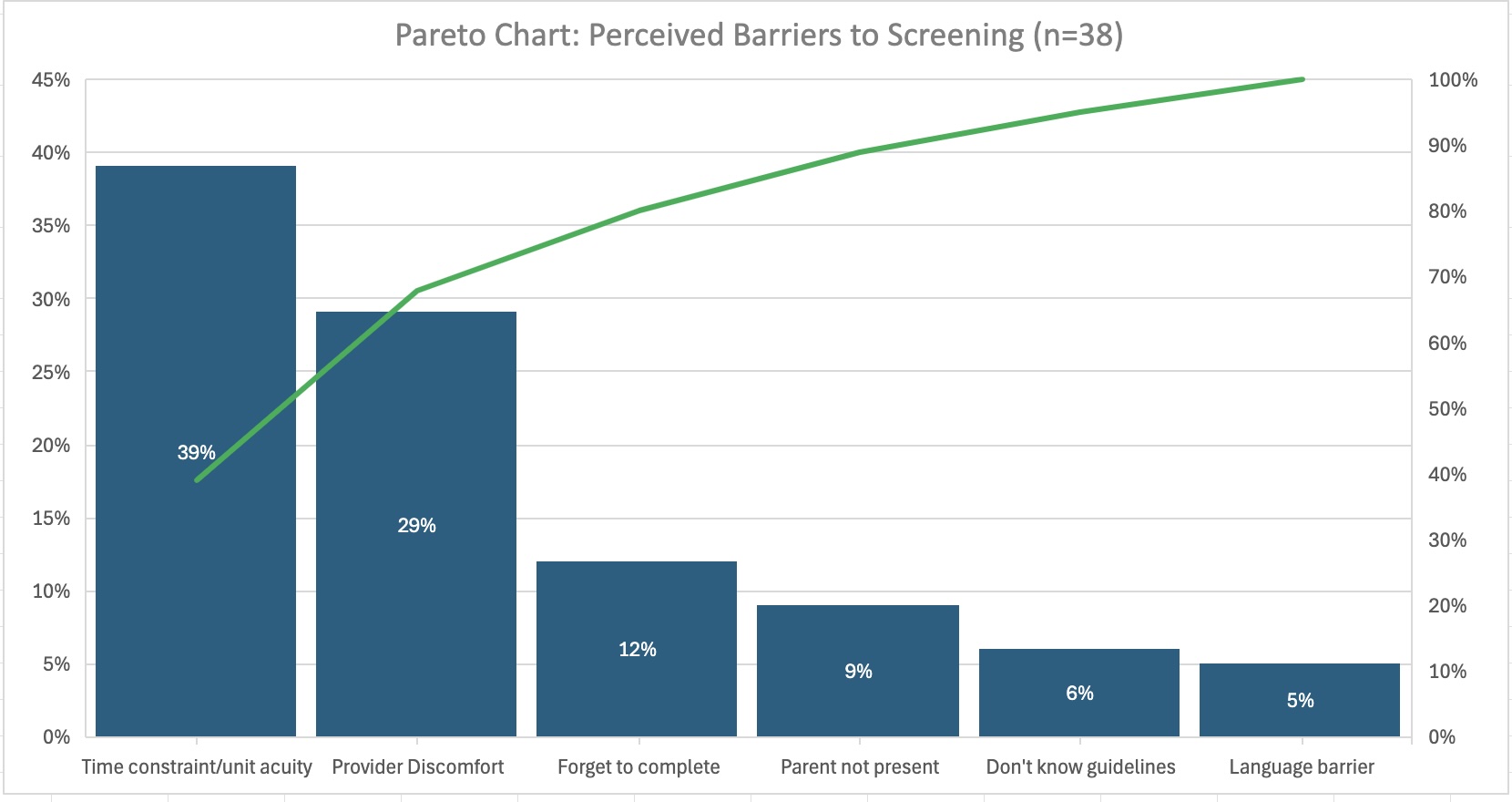 Pareto chart illustrating the barriers to completing PPD screening as reported by nurses and residents. Key concerns include prioritizing higher acuity tasks in the NICU, discomfort discussing mental health, and the tendency to forget the screening requirement.
Pareto chart illustrating the barriers to completing PPD screening as reported by nurses and residents. Key concerns include prioritizing higher acuity tasks in the NICU, discomfort discussing mental health, and the tendency to forget the screening requirement.