523 - Reduction of unplanned extubations utilizing a 3-tiered continuous improvement plan
Saturday, April 26, 2025
2:30pm - 4:45pm HST
Publication Number: 523.6284
P Sireesha. Nandula, University of Florida College of Medicine, Jacksonville, FL, United States; Edwin Soto, Wolfson Children's Hospital, Jacksonville, FL, United States; Emily Delaney, University of Florida in Jacksonville, Jacksonville, FL, United States; Amanda N.. Kreuter, Wolfson Children's Hospital, Jacksonville, FL, United States; Molly Southard, Wolfson Children's Hospital, Jacksonville, FL, United States; Amanda S. Kellum, Wolfson Children's Hospital, Jacksonville, FL, United States; Sanket D. Shah, University of Florida College of Medicine, Jackonsville, FL, United States; Vasantha HS. Kumar, University of Florida College of Medicine, Jacksonville, Jacksonville, FL, United States
Assistant Professor Unive Jacksonville, Florida, United States
Background: Unplanned extubation (UE) is a serious safety event in hospitalized children and is associated with an increased risk of airway trauma, cardiopulmonary resuscitation, and death. Historically, UEs were once considered an unfortunate consequence of care, but collaborative interdisciplinary improvement efforts have shown to be effective in reducing the UE rate. Objective: We aimed to reduce UE rate by utilizing a 3-tiered approach to UE reduction. Design/Methods: From January 2016 to May 2024, a quality improvement project was conducted in the NICU at a tertiary referral hospital in Northeast Florida. A 3-tiered approach was implemented involving a UE Drilldown Committee, a UE Workgroup, and UE Prevention Monitoring, and using methodology adapted from the Solutions for Patient Safety Collaborative. The Drilldown Committee performed timely root cause analysis with bedside team members, while the Workgroup monitored trends and monthly data and led educational initiatives, and the Prevention Monitoring Group conducted regular audits and reported deviations from best practice guidelines. We calculated the UE rate using the number of UE events and monthly ventilator days. Results: UE events (per month) decreased from a mean of 8.3 in 2016 to 4 in 2024. UE rate (events per 100 ventilator days) decreased from an average of 2.7 in January 2016 to 1.5 in June 2020. A special cause variation was noticed in June 2020, which coincided with UE workgroup formation and changing the ETT securement method. The relocation of the NICU to a newly constructed tower resulted in a temporary increase in UE rate from 1.3 in January 2022 to a high value of 4.6 in April 2022. Aggressive education resulted in UE rate Average ventilator days increased from 247.5 days per month in 2016 to 407.8 days during this period. Process measures that led to improvement included a standardized approach to endotracheal tube securement, quality of chest X-rays, and heightened monitoring of high-risk airway patients.
Conclusion(s): A methodical approach that included careful analysis of events followed by education and regular monitoring significantly reduced the UE rate in our hospital system. By treating each event as an opportunity for improvement, we sought to learn from every adverse event by implementing changes, which drove further UE rate reduction.
unplanned extubation events per ventilator days u chart depicting unplanned extubation events per ventilator days per month

 Credit")
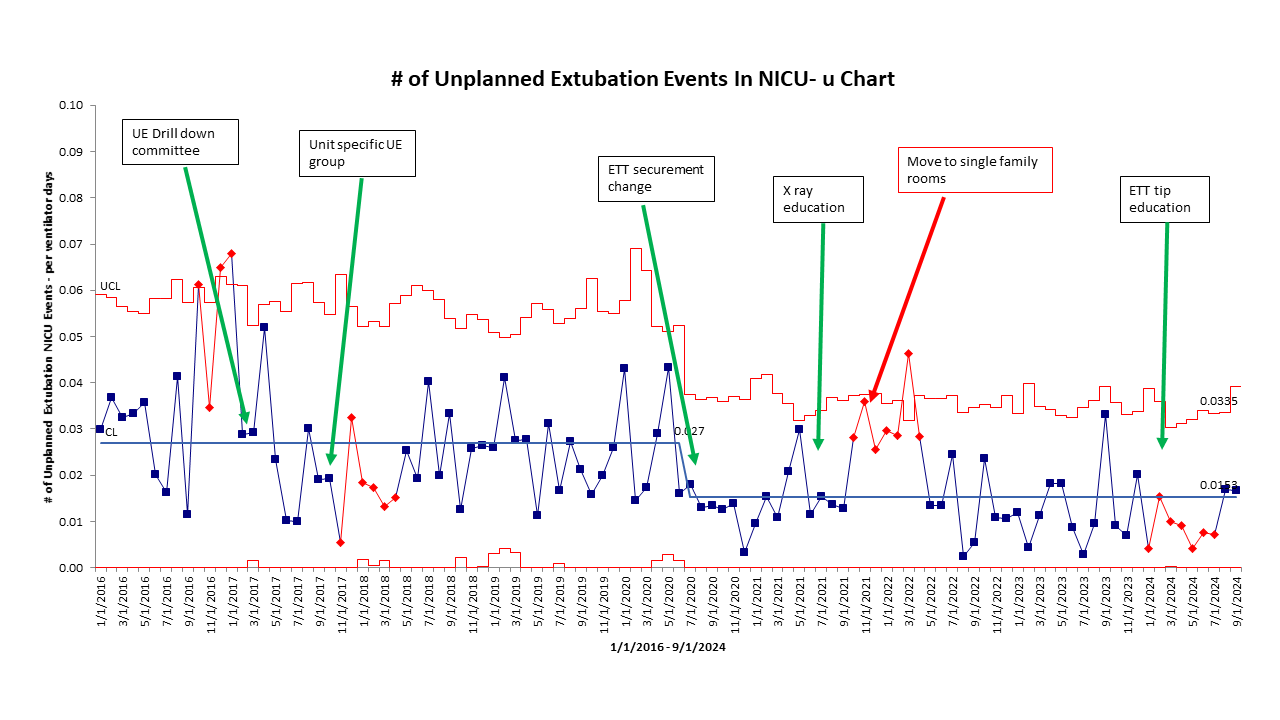 u chart depicting unplanned extubation events per ventilator days per month
u chart depicting unplanned extubation events per ventilator days per month