
Emergency Medicine 12
Session: Emergency Medicine 12
 photo")
Gabriel Devlin, MD/CM (he/him/his)
Pediatric Emergency Medicine Fellow
Children's Hospital Los Angeles
Los Angeles, California, United States
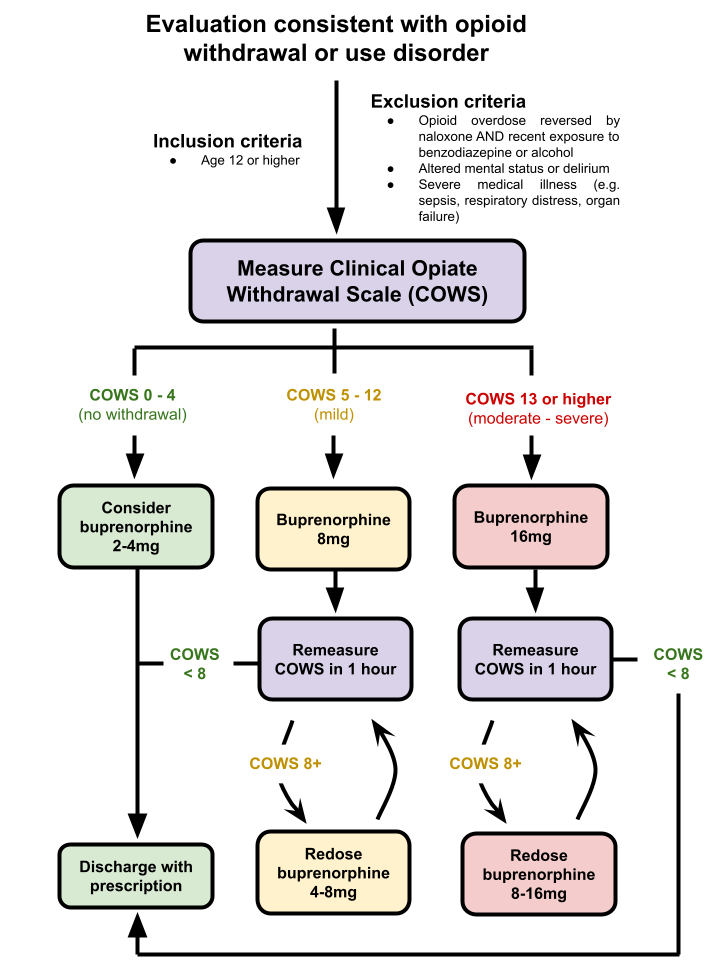 Patients presenting with symptoms of opioid withdrawal are first assessed using the Clinical Opiate Withdrawal Score (COWS) and dosed with an appropriate amount of buprenorphine. Patients are then reassessed with the COWS every hour and given additional doses of buprenorphine as needed until the COWS score decreases to less than 8. The maximum dose of buprenorphine that can be given is 32mg within 24 hours. If the patient’s symptoms are not stable after 2-3 doses of buprenorphine (or the maximum dose is reached), clinicians consider admission to the hospital.
Patients presenting with symptoms of opioid withdrawal are first assessed using the Clinical Opiate Withdrawal Score (COWS) and dosed with an appropriate amount of buprenorphine. Patients are then reassessed with the COWS every hour and given additional doses of buprenorphine as needed until the COWS score decreases to less than 8. The maximum dose of buprenorphine that can be given is 32mg within 24 hours. If the patient’s symptoms are not stable after 2-3 doses of buprenorphine (or the maximum dose is reached), clinicians consider admission to the hospital.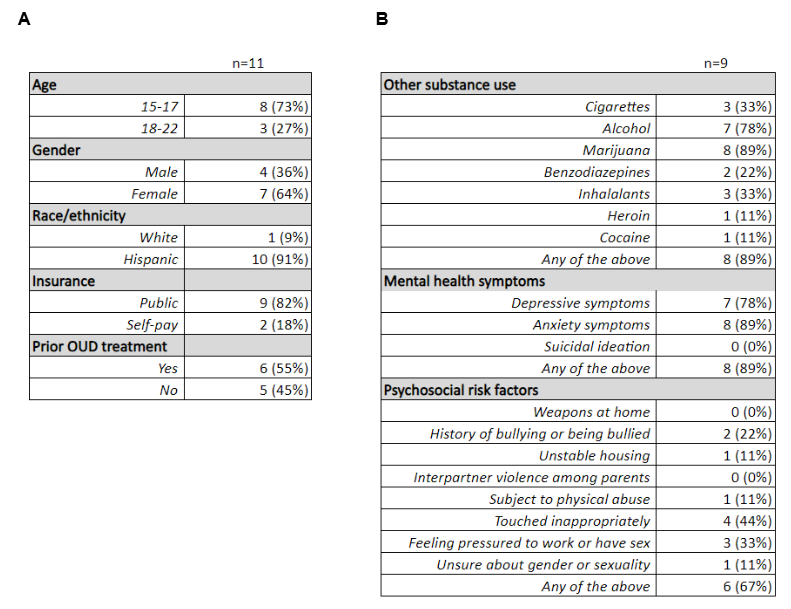 (A) Demographic characteristics of the 11 patients that met inclusion criteria for the study.
(A) Demographic characteristics of the 11 patients that met inclusion criteria for the study. 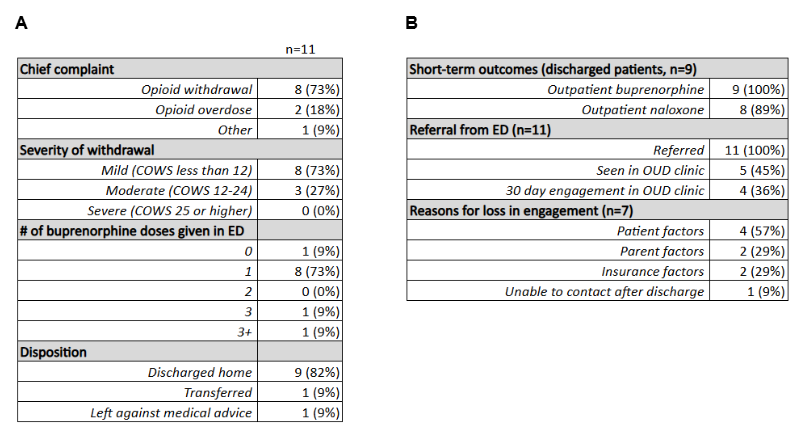 (A) Treatment characteristics among ED patients induced with buprenorphine for opioid withdrawal.Patients presenting with symptoms of opioid withdrawal are first assessed using the Clinical Opiate Withdrawal Score (COWS) and dosed with an appropriate amount of buprenorphine. Patients are then reassessed with the COWS every hour and given additional doses of buprenorphine as needed until the COWS score decreases to less than 8. The maximum dose of buprenorphine that can be given is 32mg within 24 hours. If the patient’s symptoms are not stable after 2-3 doses of buprenorphine (or the maximum dose is reached), clinicians consider admission to the hospital.(A) Demographic characteristics of the 11 patients that met inclusion criteria for the study. (A) Treatment characteristics among ED patients induced with buprenorphine for opioid withdrawal.
(A) Treatment characteristics among ED patients induced with buprenorphine for opioid withdrawal.Patients presenting with symptoms of opioid withdrawal are first assessed using the Clinical Opiate Withdrawal Score (COWS) and dosed with an appropriate amount of buprenorphine. Patients are then reassessed with the COWS every hour and given additional doses of buprenorphine as needed until the COWS score decreases to less than 8. The maximum dose of buprenorphine that can be given is 32mg within 24 hours. If the patient’s symptoms are not stable after 2-3 doses of buprenorphine (or the maximum dose is reached), clinicians consider admission to the hospital.(A) Demographic characteristics of the 11 patients that met inclusion criteria for the study. (A) Treatment characteristics among ED patients induced with buprenorphine for opioid withdrawal.