Emergency Medicine 4
Session: Emergency Medicine 4
Justine Lam, B.S. (she/her/hers)
Master's Student
University of Rochester School of Medicine and Dentistry
Rochester, New York, United States
.png)
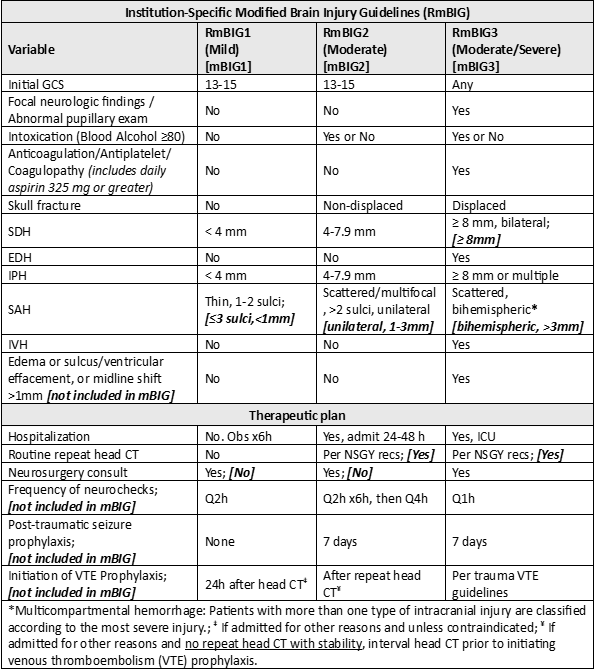 In places where the institution-specific guidelines deviate from existing modified brain injury guidelines (mBIG)6,7, the relevant mBIG criteria are shown in brackets.
In places where the institution-specific guidelines deviate from existing modified brain injury guidelines (mBIG)6,7, the relevant mBIG criteria are shown in brackets.