682 - Normative Values of Glucose-6-Phosphate Dehydrogenase (G6PD) in Preterm Infants
Monday, April 28, 2025
7:00am - 9:15am HST
Publication Number: 682.6000
Shana Yazdanpanah, Staten Island University Hospital, Staten Island, NY, United States; Jonathan Blau, Cohen Children's Medical Center - Staten Island University Hospital, Staten Island, NY, United States; Eleny Romanos-Sirakis, SIUH Northwell Health, SI, NY, United States; Un Jung Lee, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, New Hyde Park, NY, United States
Staten Island University Hospital Staten Island, New York, United States
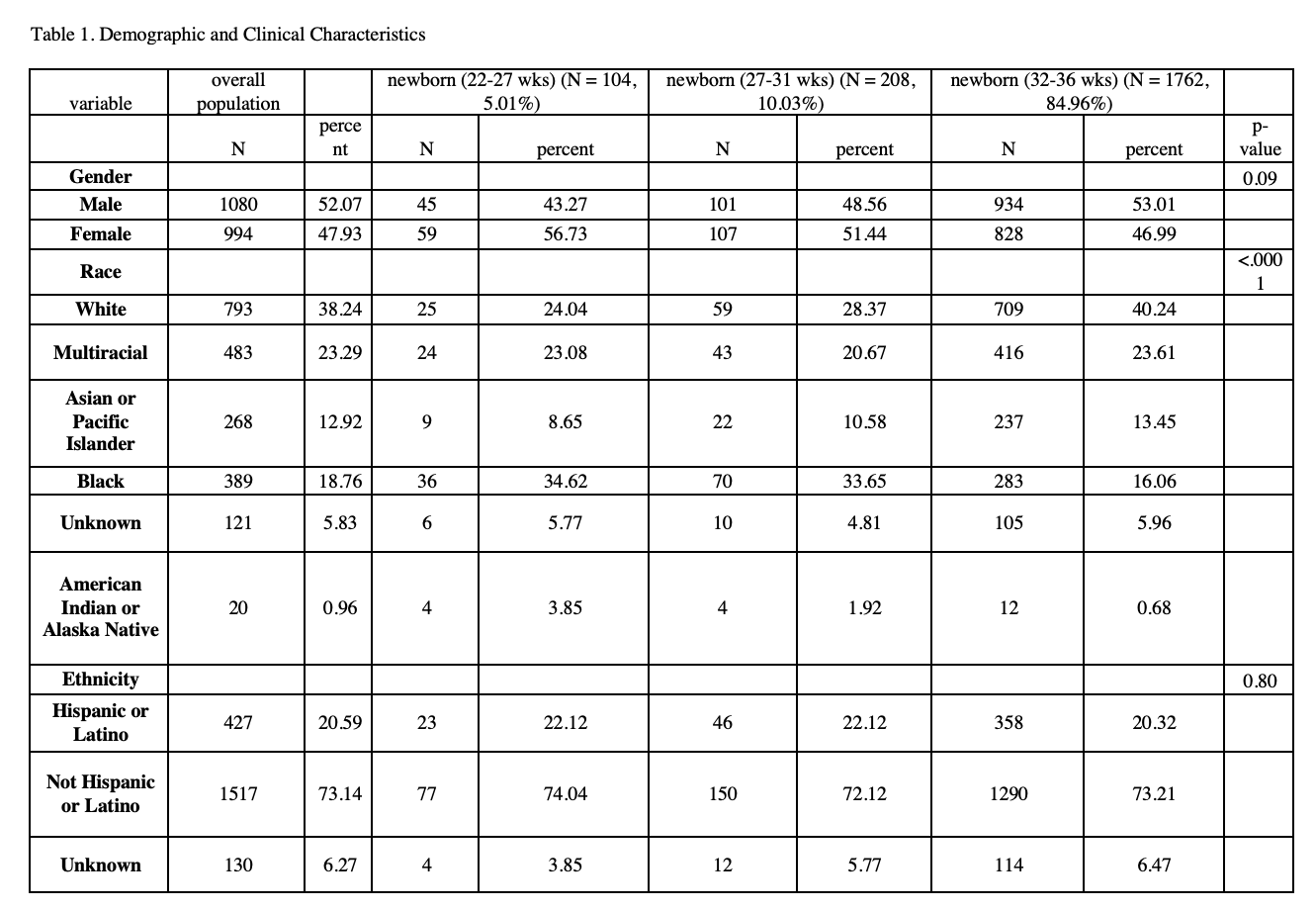
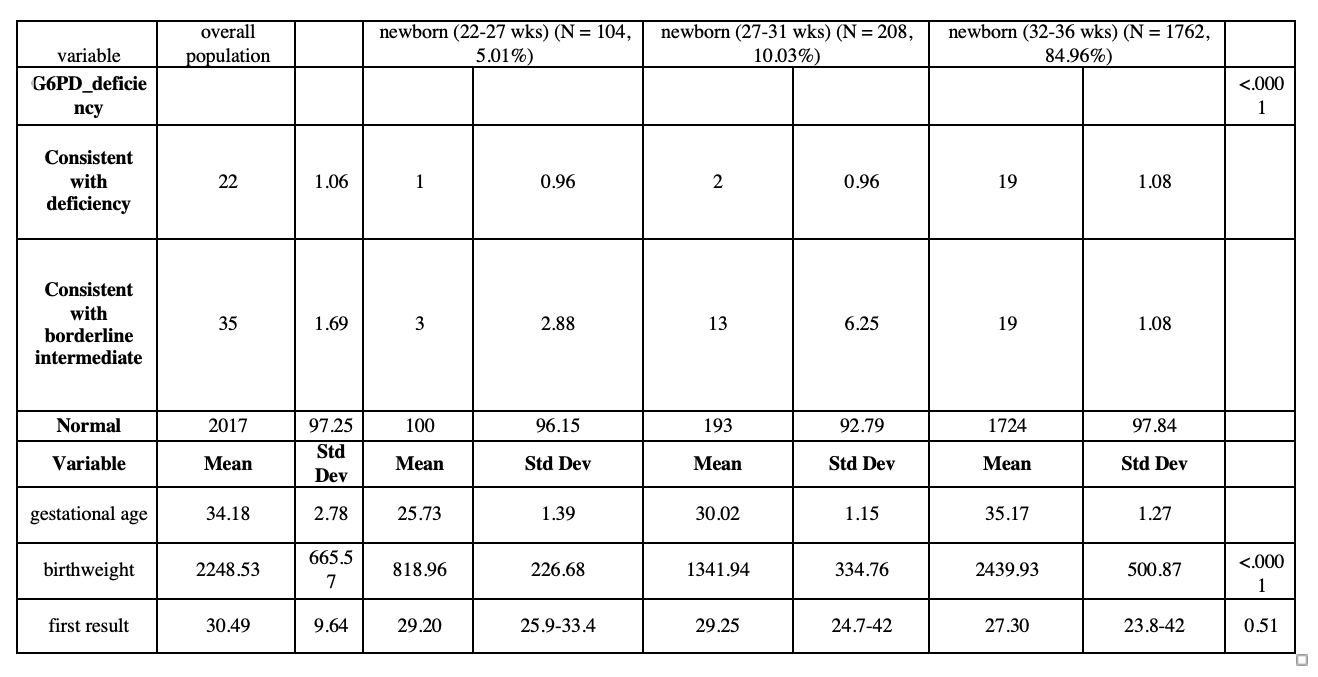
Background: Preterm infants are particularly susceptible to oxidative damage secondary to G6PD deficiency. However, there has been limited research on the normative values in preterm infants. In 2022, New York State recommended universal newborn G6PD screening. This presented an opportunity to evaluate normative G6PD values in the preterm population. Objective: To assess normative values of G6PD across varying gestational ages in preterm infants as well as secondary variables such as gender, race, ethnicity, and birth weight. Design/Methods: In this study, we used a retrospective cohort design to extract data from the electronic medical records (EMRs) of 2076 preterm infants born within 7 Northwell birthing centers between July 1st, 2022, and June 30th, 2023, after New York State recommended universal newborn G6PD screening. Statistical analyses were conducted using SASV9.4 to primarily explore the relationship between G6PD values and gestational age. Further analyses were conducted to include gender, race, ethnicity, and birth weight as associated variables. Comparisons between groups were carried out using either ANOVA or Wilcoxon test for continuous variables; and chi-squared or Fisher’s exact test for categorical variables. Results: Of the 2076 preterm infants assessed in this study, 46 were found to have levels consistent with G6PD deficiency. There was no significant difference in G6PD values when stratified by gestational age. Preterm groups were divided by gestational age as such; 1) preterm newborns born at 22 – 27 weeks; N= 104, 2) preterm newborns group (27 – 31 weeks; N=208, and 3) preterm newborn born at 32 – 36 weeks; N= 1762. Table 1 provides the descriptive and inferential statistics for demographic characteristics and physiological variables by group. There were significant differences between preterm newborn groups with respect to birthing center site, gender, race, G6PD deficiency category, and birth weight. Figure 1 shows the bar graph of the proportion of G6PD deficiency according to preterm groups and figure 2 shows the distribution of G6PD for all preterms and those divided among the 3 preterm groups.
Conclusion(s): The extrapolation of normative G6PD enzymatic values from data derived from term infants, while resourceful may provide an inaccurate representation of the complex physiologic differences with decreased gestational age. Understanding the baseline levels of this vital enzyme in preterm infants is crucial for diagnosing and managing potential G6PD-related hemolytic anemia and subsequent kernicterus, thus optimizing neonatal care.
Proportion of G6PD Deficiency According to Preterm Groups

.png)