
Neonatal GI Physiology & NEC 4
Session: Neonatal GI Physiology & NEC 4
Sarah Z. Wang, MD, MPH (she/her/hers)
Research Fellow
Boston Children's Hospital
Boston, Massachusetts, United States
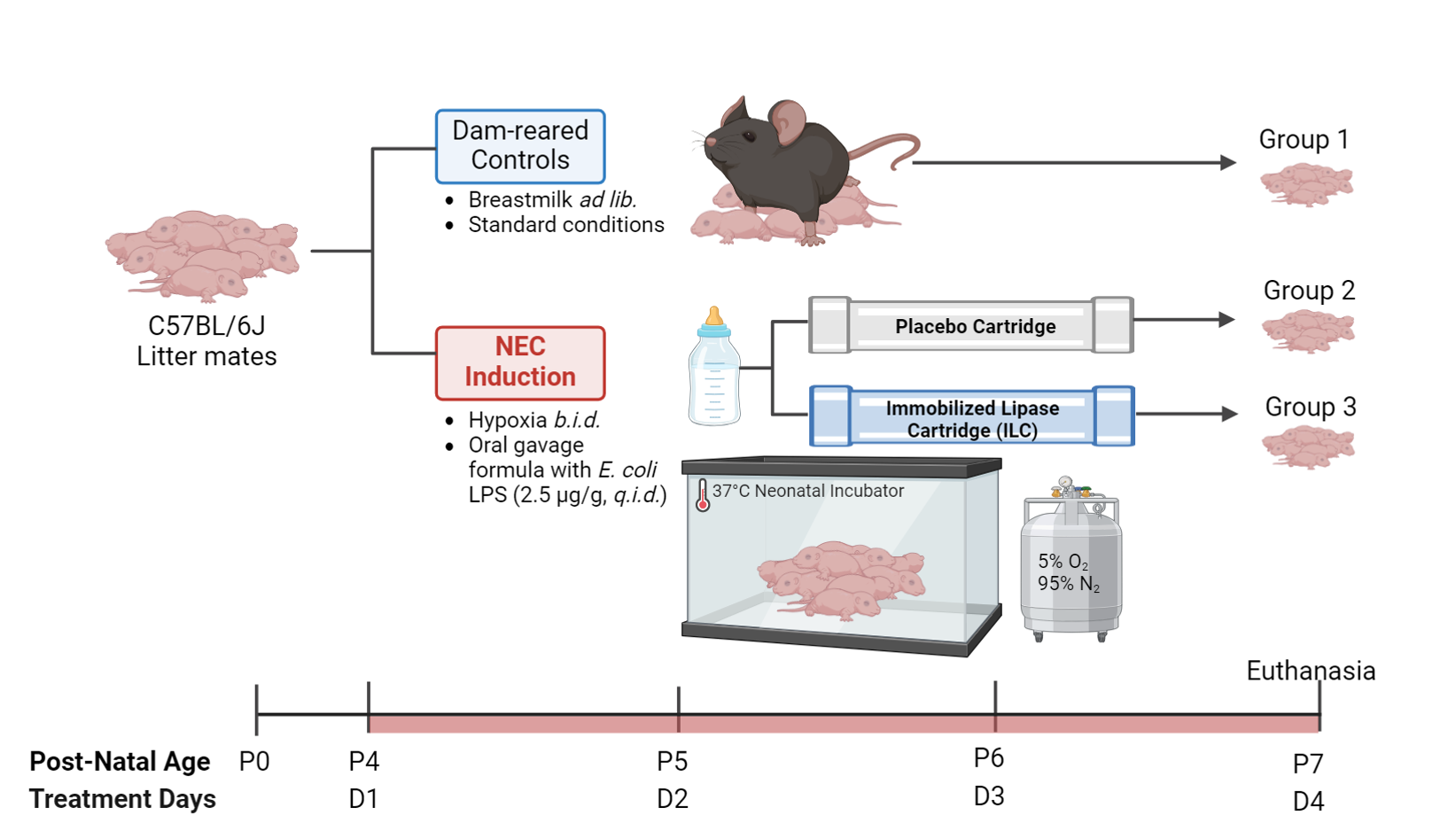 Figure 1. Experimental design investigating the effects of enteral formula pre-digested by an Immobilized Lipase Cartridge in a necrotizing enterocolitis mouse model. Group 1 are breastmilk-fed controls. Groups 2 and 3 undergo experimental induction of NEC via a combination of oral gavage feeding with formula containing E. coli-derived lipopolysaccharide (2.5 ug/g) and twice-daily hypoxia exposure from post-natal day 4 through 6 as described previously (Nolan et al., STAR Protoc, 2021). Group 2 receives formula processed through an empty, placebo cartridge. Group 3 receives formula pre-digested by the ILC. Animals are sacrificed on P7. NEC – necrotizing enterocolitis; ILC – Immobilized Lipase Cartridge; ad lib – ad libitum (liberally); q.i.d. – four times per day.
Figure 1. Experimental design investigating the effects of enteral formula pre-digested by an Immobilized Lipase Cartridge in a necrotizing enterocolitis mouse model. Group 1 are breastmilk-fed controls. Groups 2 and 3 undergo experimental induction of NEC via a combination of oral gavage feeding with formula containing E. coli-derived lipopolysaccharide (2.5 ug/g) and twice-daily hypoxia exposure from post-natal day 4 through 6 as described previously (Nolan et al., STAR Protoc, 2021). Group 2 receives formula processed through an empty, placebo cartridge. Group 3 receives formula pre-digested by the ILC. Animals are sacrificed on P7. NEC – necrotizing enterocolitis; ILC – Immobilized Lipase Cartridge; ad lib – ad libitum (liberally); q.i.d. – four times per day.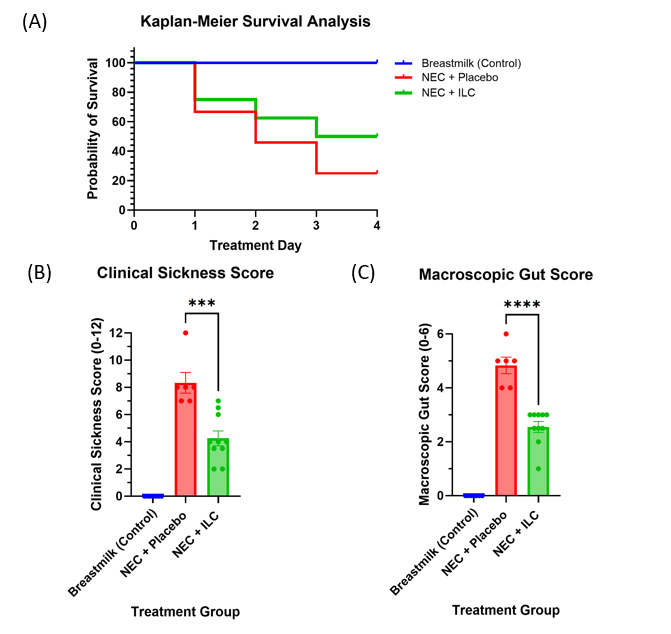 Figure 2. Survival and clinical outcomes in a necrotizing enterocolitis mouse model. (A) Survival analysis; (B) Clinical sickness score; (C) Macroscopic gut score. Two independent masked observers assessed clinical sickness and macroscopic gut scores on day of euthanasia according to a validated NEC severity scoring system (Zani et al., Eur J Pediatr Surg, 2008). Values are expressed as the mean +/- standard error of the mean (SEM). NEC – necrotizing enterocolitis; ILC – Immobilized Lipase Cartridge.
Figure 2. Survival and clinical outcomes in a necrotizing enterocolitis mouse model. (A) Survival analysis; (B) Clinical sickness score; (C) Macroscopic gut score. Two independent masked observers assessed clinical sickness and macroscopic gut scores on day of euthanasia according to a validated NEC severity scoring system (Zani et al., Eur J Pediatr Surg, 2008). Values are expressed as the mean +/- standard error of the mean (SEM). NEC – necrotizing enterocolitis; ILC – Immobilized Lipase Cartridge.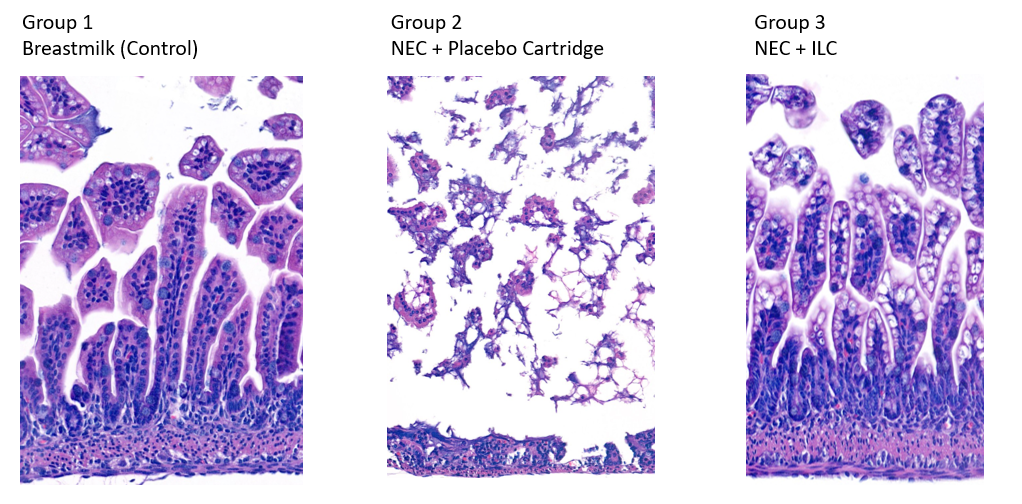 Figure 3. Representative H&E-stained terminal ileum specimens in a necrotizing enterocolitis mouse model. Group 1 – breastmilk-fed neonatal mice had normal villus architecture. Group 2 – NEC mice fed formula processed through a placebo cartridge had villus sloughing and disrupted basement membrane. Group 3 – NEC mice fed formula processed through the ILC had preserved villus architecture. 10X magnification. NEC – necrotizing enterocolitis; ILC – Immobilized Lipase Cartridge.
Figure 3. Representative H&E-stained terminal ileum specimens in a necrotizing enterocolitis mouse model. Group 1 – breastmilk-fed neonatal mice had normal villus architecture. Group 2 – NEC mice fed formula processed through a placebo cartridge had villus sloughing and disrupted basement membrane. Group 3 – NEC mice fed formula processed through the ILC had preserved villus architecture. 10X magnification. NEC – necrotizing enterocolitis; ILC – Immobilized Lipase Cartridge.