
Neonatal/Infant Resuscitation 3
Session: Neonatal/Infant Resuscitation 3
 (she/her/hers) photo")
Ebony R. Cannata, BSc (hons) (she/her/hers)
PhD Candidate
The Ritchie Centre, Hudson Institute of Medical Research
Leongatha, Victoria, Australia
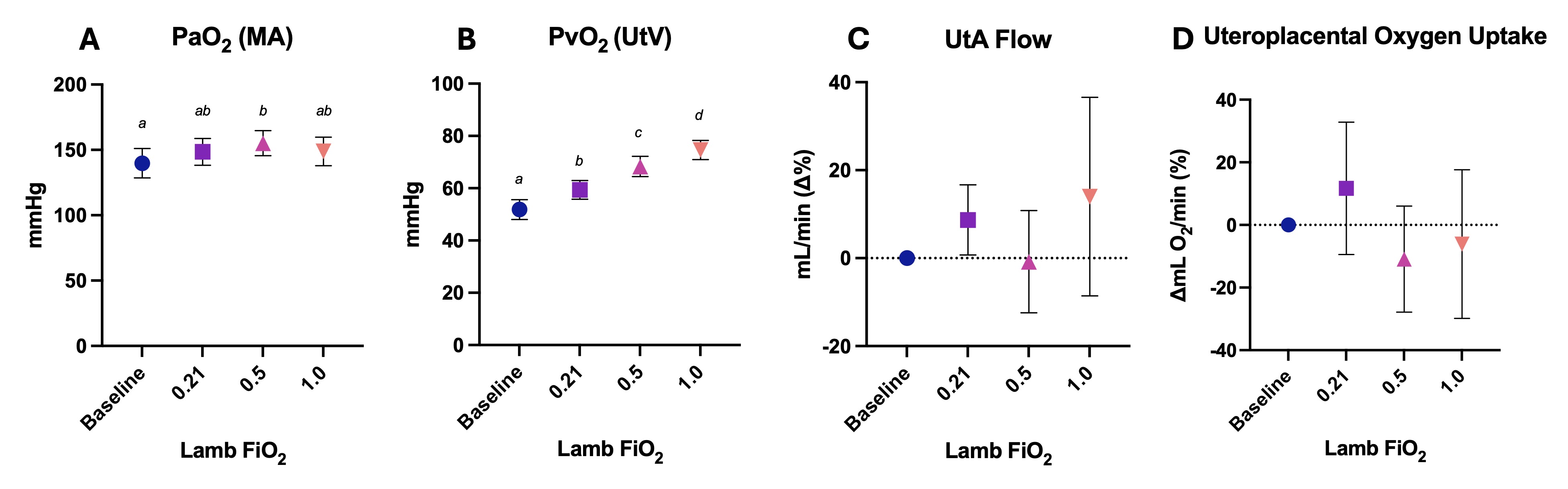 A) Partial pressure of oxygen (PaO2) in maternal arterial (MA) blood, B) partial pressure of oxygen (PvO2) in uterine venous (UtV) blood, C) uterine artery (UtA) blood flow, and D) and uteroplacental oxygen uptake during ventilation of lambs with different fraction of inspired oxygen (FiO2) levels. Uteroplacental oxygen uptake was calculated by multiplying the difference between MA and UtV oxygen content by UtA blood flow. Data are presented as mean ± SEM. Values that do not share a common letter are significantly different from each other (p < 0.05).
A) Partial pressure of oxygen (PaO2) in maternal arterial (MA) blood, B) partial pressure of oxygen (PvO2) in uterine venous (UtV) blood, C) uterine artery (UtA) blood flow, and D) and uteroplacental oxygen uptake during ventilation of lambs with different fraction of inspired oxygen (FiO2) levels. Uteroplacental oxygen uptake was calculated by multiplying the difference between MA and UtV oxygen content by UtA blood flow. Data are presented as mean ± SEM. Values that do not share a common letter are significantly different from each other (p < 0.05)..jpg) A) Partial pressure of oxygen (PvO2) in umbilical venous (UmbV) blood, B) partial pressure of oxygen (PaO2) in femoral arterial (FA) blood, C) UmbV blood flow, and D) and fetal oxygen uptake during ventilation of lambs with different fraction of inspired oxygen (FiO2) levels. Fetal oxygen uptake was calculated by multiplying the difference between UmbV and FA oxygen content, by UmbV blood flow. Data are presented as mean ± SEM. Values that do not share a common letter are significantly different from each other (p < 0.05).
A) Partial pressure of oxygen (PvO2) in umbilical venous (UmbV) blood, B) partial pressure of oxygen (PaO2) in femoral arterial (FA) blood, C) UmbV blood flow, and D) and fetal oxygen uptake during ventilation of lambs with different fraction of inspired oxygen (FiO2) levels. Fetal oxygen uptake was calculated by multiplying the difference between UmbV and FA oxygen content, by UmbV blood flow. Data are presented as mean ± SEM. Values that do not share a common letter are significantly different from each other (p < 0.05).