
Mental Health 4
Session: Mental Health 4
Cory Alexieff, DO (he/him/his)
Pediatric Hospital Medicine Fellow
K. Hovnanian Children's Hospital at Jersey Shore University Medical Center
Red Bank, New Jersey, United States
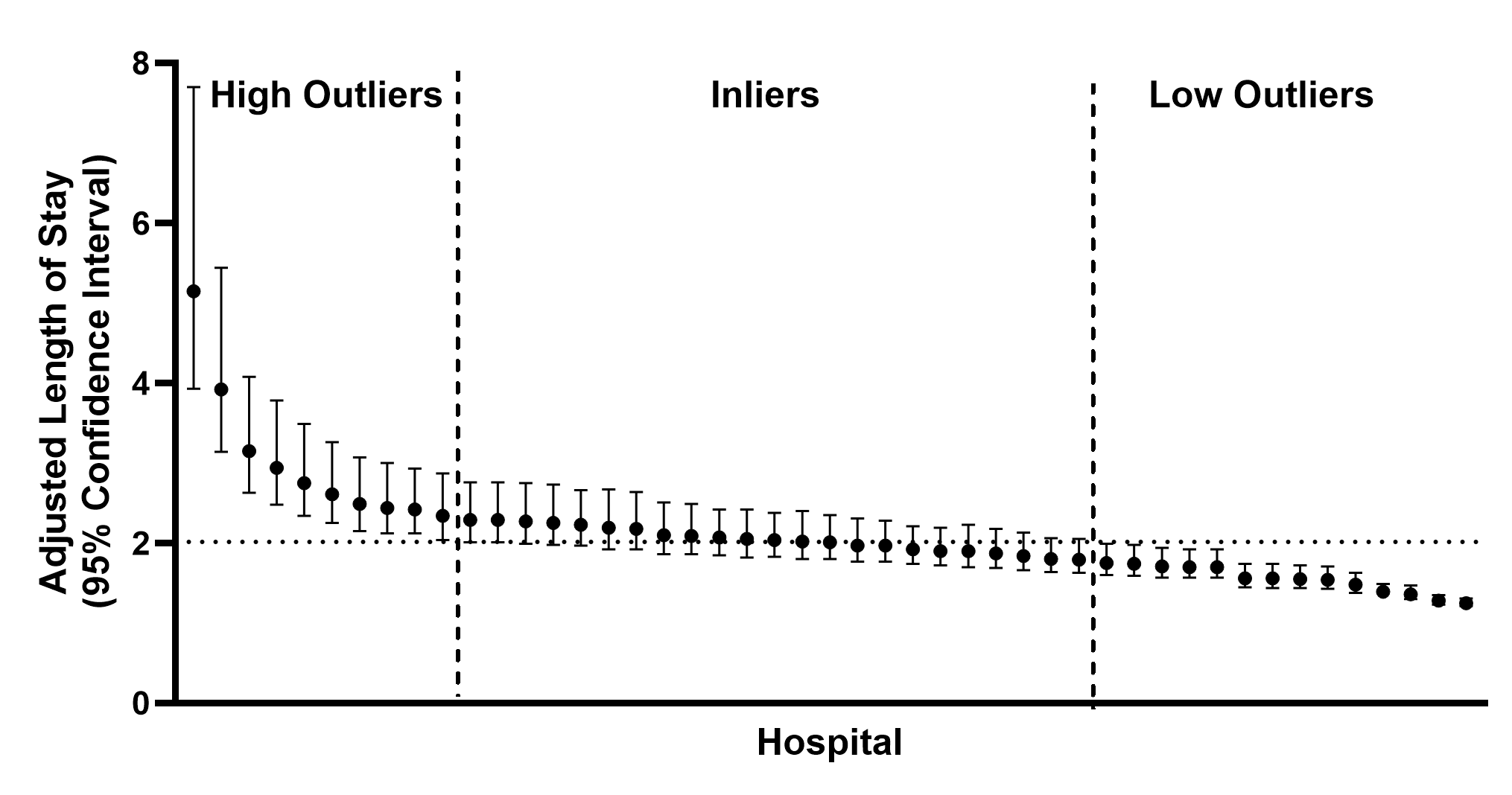 Length of Stay measured in days. Each data point represents a unique PHIS-reporting hospital. Horizontal dotted line represents grand mean across all hospitals.
Length of Stay measured in days. Each data point represents a unique PHIS-reporting hospital. Horizontal dotted line represents grand mean across all hospitals..png) Length of Stay measured in days. Qualitative factors were dichotomized for the presence or absence of each item. Quantitative factors were dichotomized into “high” and “low” categories based on their relation to the median value amongst all hospitals. For example, median Medicaid Revenue was 54.2% and values above this were counted as “High Percent Medicaid Revenue”. FTE: full-time equivalent. AOM: adjusted occupied bed.
Length of Stay measured in days. Qualitative factors were dichotomized for the presence or absence of each item. Quantitative factors were dichotomized into “high” and “low” categories based on their relation to the median value amongst all hospitals. For example, median Medicaid Revenue was 54.2% and values above this were counted as “High Percent Medicaid Revenue”. FTE: full-time equivalent. AOM: adjusted occupied bed.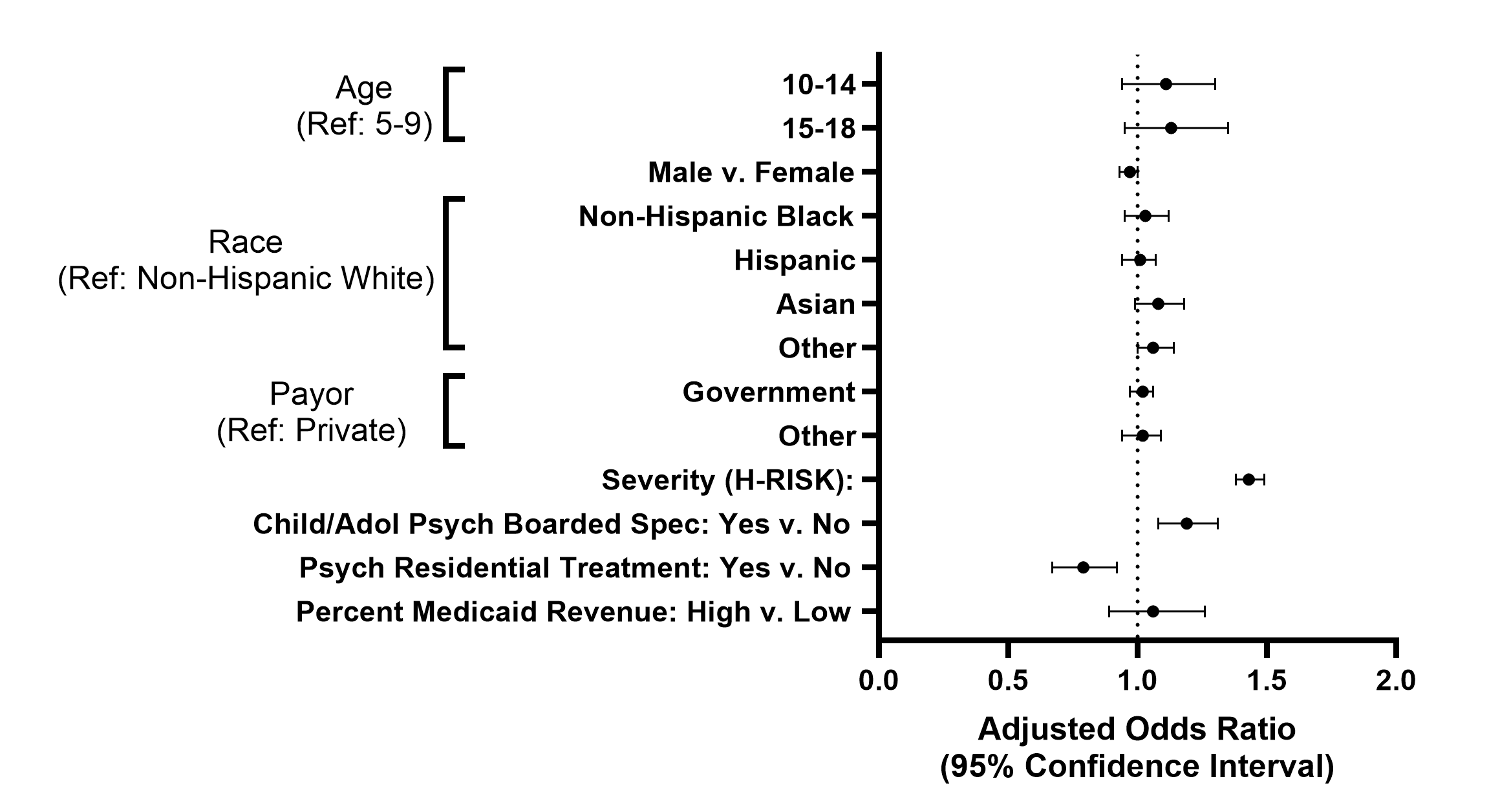 Length of Stay measured in days. Each data point represents a unique PHIS-reporting hospital. Horizontal dotted line represents grand mean across all hospitals.Length of Stay measured in days. Qualitative factors were dichotomized for the presence or absence of each item. Quantitative factors were dichotomized into “high” and “low” categories based on their relation to the median value amongst all hospitals. For example, median Medicaid Revenue was 54.2% and values above this were counted as “High Percent Medicaid Revenue”. FTE: full-time equivalent. AOM: adjusted occupied bed.
Length of Stay measured in days. Each data point represents a unique PHIS-reporting hospital. Horizontal dotted line represents grand mean across all hospitals.Length of Stay measured in days. Qualitative factors were dichotomized for the presence or absence of each item. Quantitative factors were dichotomized into “high” and “low” categories based on their relation to the median value amongst all hospitals. For example, median Medicaid Revenue was 54.2% and values above this were counted as “High Percent Medicaid Revenue”. FTE: full-time equivalent. AOM: adjusted occupied bed.