
Neonatal Pulmonology - Basic/Translational Science 3
Session: Neonatal Pulmonology - Basic/Translational Science 3
.jpg "Ana H. Martinez, MD (she/her/hers) photo")
Ana H. Martinez, MD (she/her/hers)
Fellow
Johns Hopkins All Children's Hospital
St. Petersburg, Florida, United States
.png) Demographic and outcomes comparing neonates who had a diagnosis of grade 2/3 BPD and those who had no BPD (grade 0) or grade 1 BPD. GA: gestational age; BW: birth weight; SC: systemic corticosteroids; cGA: corrected gestational age; DOL: day of life.
Demographic and outcomes comparing neonates who had a diagnosis of grade 2/3 BPD and those who had no BPD (grade 0) or grade 1 BPD. GA: gestational age; BW: birth weight; SC: systemic corticosteroids; cGA: corrected gestational age; DOL: day of life.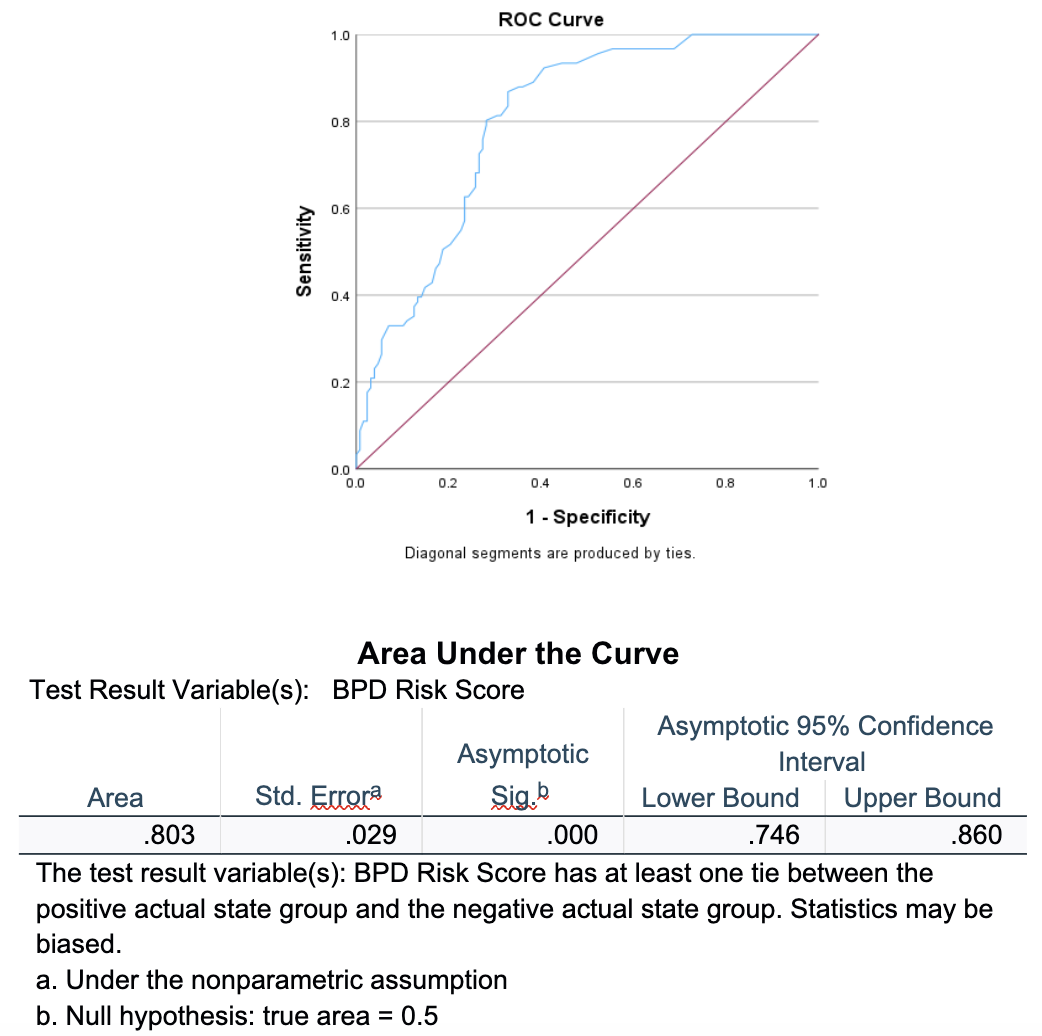 ROC curve showing NICHD BPD risk estimation of grade 2 and 3 BPD and death as a predictor of actual development of the disease.
ROC curve showing NICHD BPD risk estimation of grade 2 and 3 BPD and death as a predictor of actual development of the disease..png) Boxplots of both groups 0= BPD grade 0/1 and 1= BPD grade 2/3/ Death. Around 73% of the patients in group 0 fall under 40% risk and around 36% of group 1 patients fall under the 40% cut off, however most of group 1 patients fall under 60% (around 66%).
Boxplots of both groups 0= BPD grade 0/1 and 1= BPD grade 2/3/ Death. Around 73% of the patients in group 0 fall under 40% risk and around 36% of group 1 patients fall under the 40% cut off, however most of group 1 patients fall under 60% (around 66%). 