
Critical Care 4
Session: Critical Care 4
 photo")
Constance E. Poplos, MS (she/her/hers)
student
University of Tennessee Health Science Center College of Medicine
Memphis, Tennessee, United States
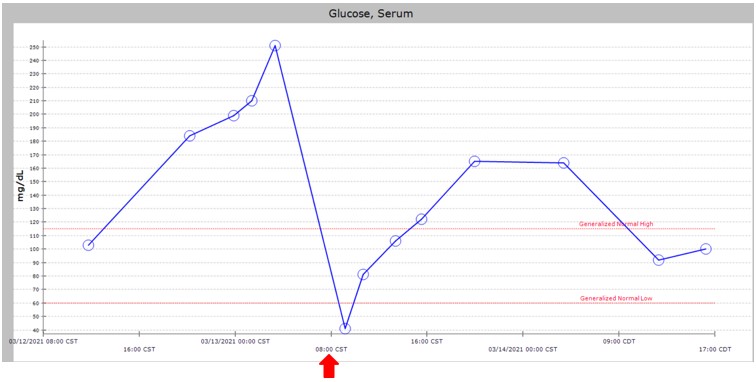 Example of Hypoglycemic Event: Patient weight 2.5 kg, Citrate Rate 75 ml/hr citrate. Provided GIR 12 mg/kg/min with abrupt cessation at 800am (marked with red arrow).
Example of Hypoglycemic Event: Patient weight 2.5 kg, Citrate Rate 75 ml/hr citrate. Provided GIR 12 mg/kg/min with abrupt cessation at 800am (marked with red arrow).