
Genomics/Epigenomics 1
Session: Genomics/Epigenomics 1
 photo")
Tanner Ellsworth, MD, MPH (he/him/his)
Neonatal-Perinatal Medicine Fellow
University of Utah
Salt Lake City, Utah, United States
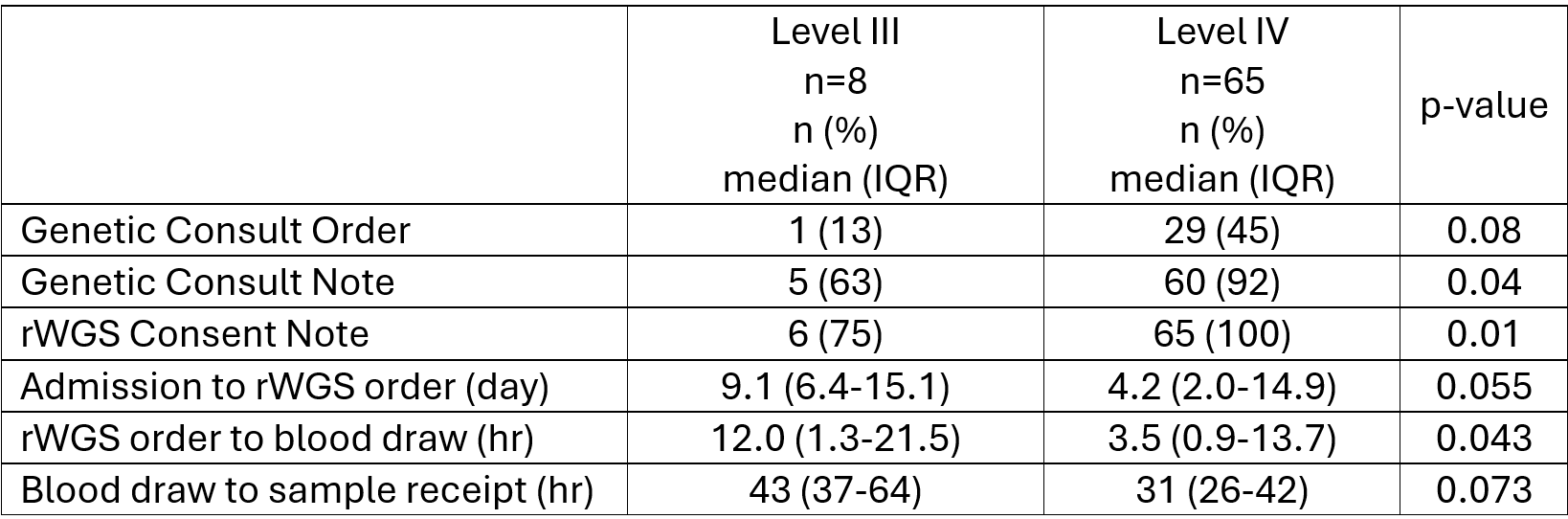 Comparison of rWGS processing in Level III vs. Level IV settings
Comparison of rWGS processing in Level III vs. Level IV settings