Critical Care 2
Session: Critical Care 2
Jefferson Bedell, II, MD (he/him/his)
Associate Professor
UTMB
Houston, Texas, United States
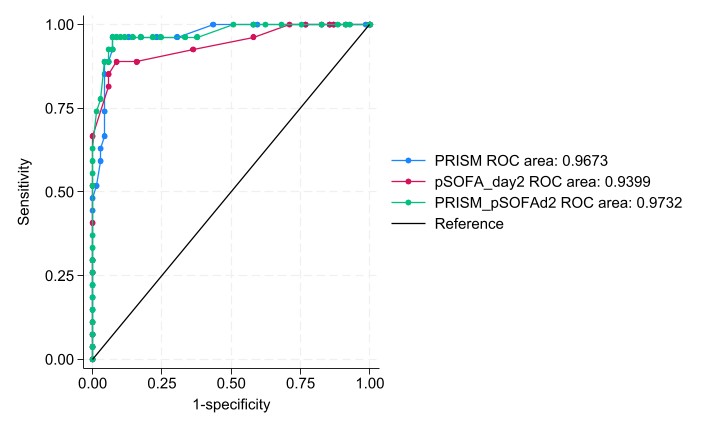
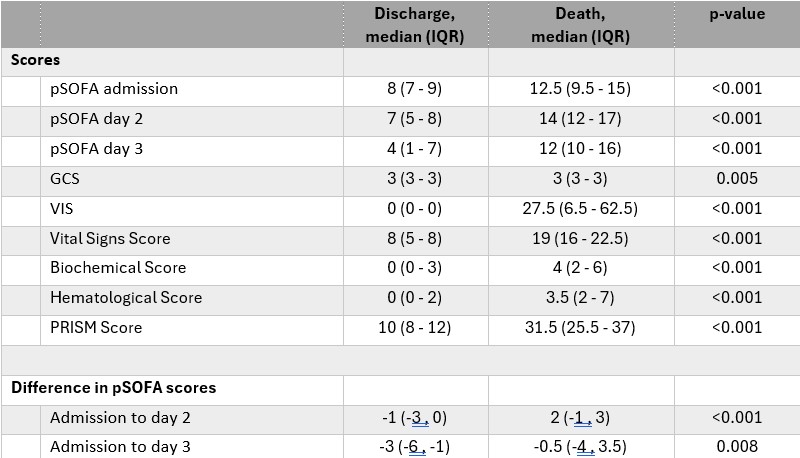 pediatric Sequential Organ Failure Assessment score (pSOFA); GCS, glascow coma scale; VIS, vaso-inotropic support; Pediatric Risk of Mortality (PRSIM) III at 24hrs
pediatric Sequential Organ Failure Assessment score (pSOFA); GCS, glascow coma scale; VIS, vaso-inotropic support; Pediatric Risk of Mortality (PRSIM) III at 24hrs 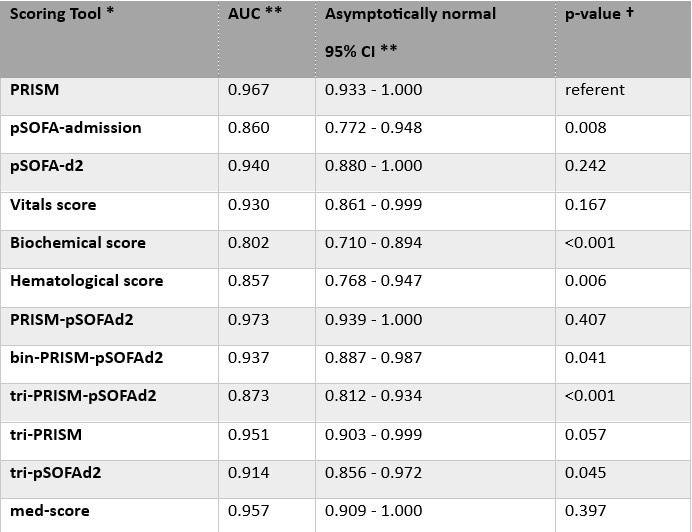 * Description of each of the scores is listed in the body of the results document
* Description of each of the scores is listed in the body of the results document