
Allergy, Immunology, and Rheumatology 2
Session: Allergy, Immunology, and Rheumatology 2
 photo")
Ernestina Hansen-Sackey, MD MSC (she/her/hers)
Pediatric Resident Physician
Valley Children's Healthcare
Madera, Texas, United States
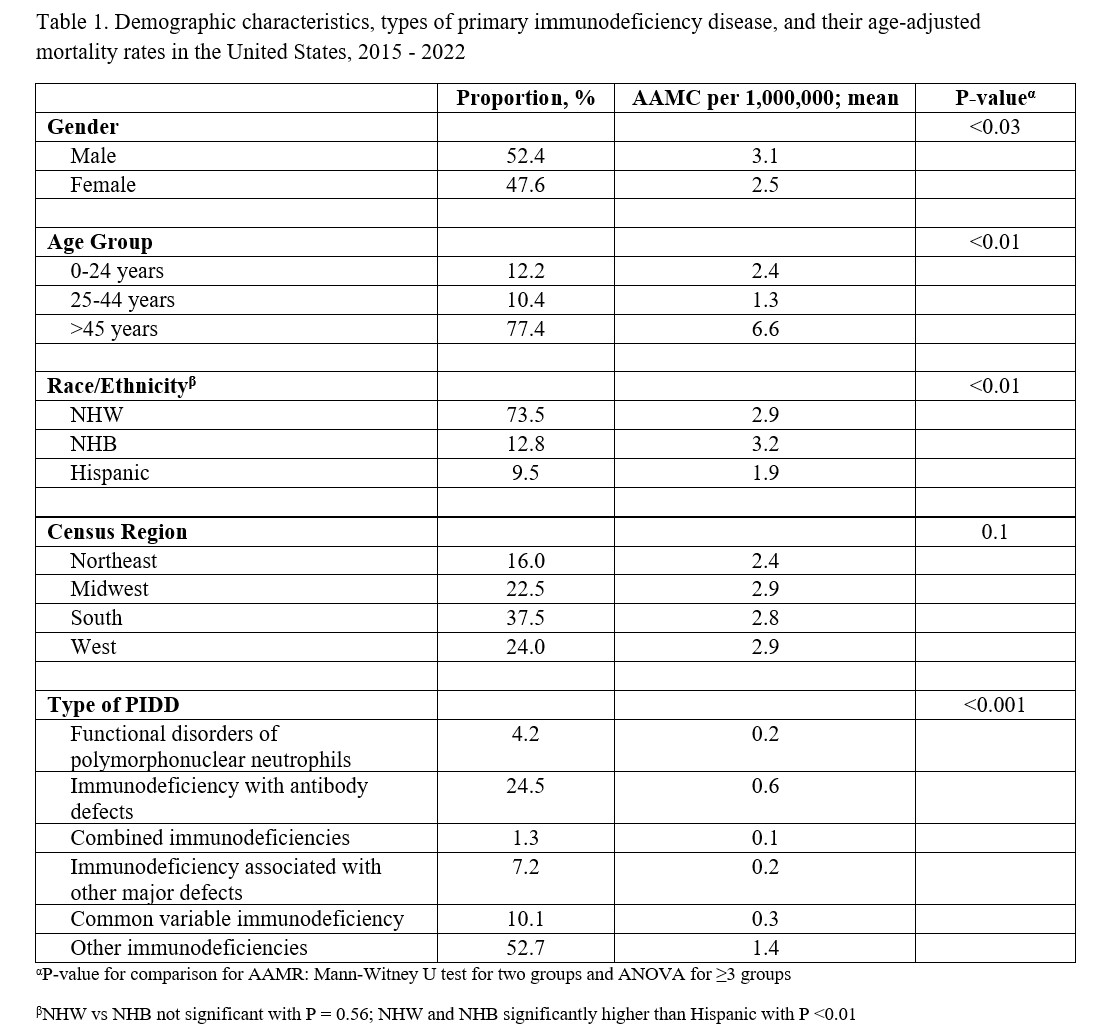 Demographic characteristics, types of primary immunodeficiency disease, and their age-adjusted mortality rates in the United States, 2015 - 2022
Demographic characteristics, types of primary immunodeficiency disease, and their age-adjusted mortality rates in the United States, 2015 - 2022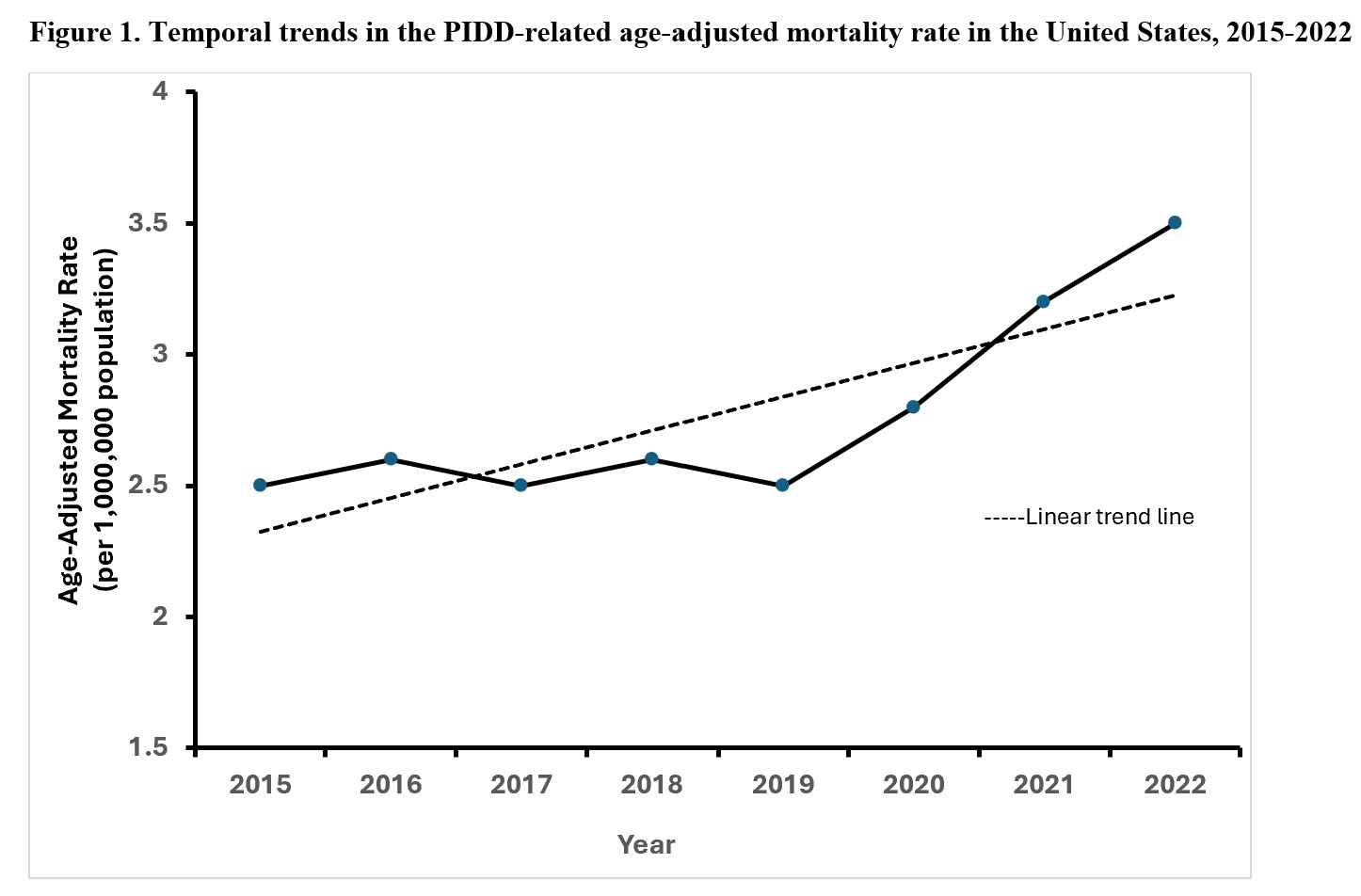 Temporal trends in the PIDD-related age-adjusted mortality rate in the United States, 2015-2022Demographic characteristics, types of primary immunodeficiency disease, and their age-adjusted mortality rates in the United States, 2015 - 2022Temporal trends in the PIDD-related age-adjusted mortality rate in the United States, 2015-2022
Temporal trends in the PIDD-related age-adjusted mortality rate in the United States, 2015-2022Demographic characteristics, types of primary immunodeficiency disease, and their age-adjusted mortality rates in the United States, 2015 - 2022Temporal trends in the PIDD-related age-adjusted mortality rate in the United States, 2015-2022