
Neonatal Quality Improvement 2
Session: Neonatal Quality Improvement 2
 photo")
Emiko Yamada, MD (she/her/hers)
Resident
Comer Children's Hospital at University of Chicago Medical Center
Chicago, Illinois, United States
.jpg)
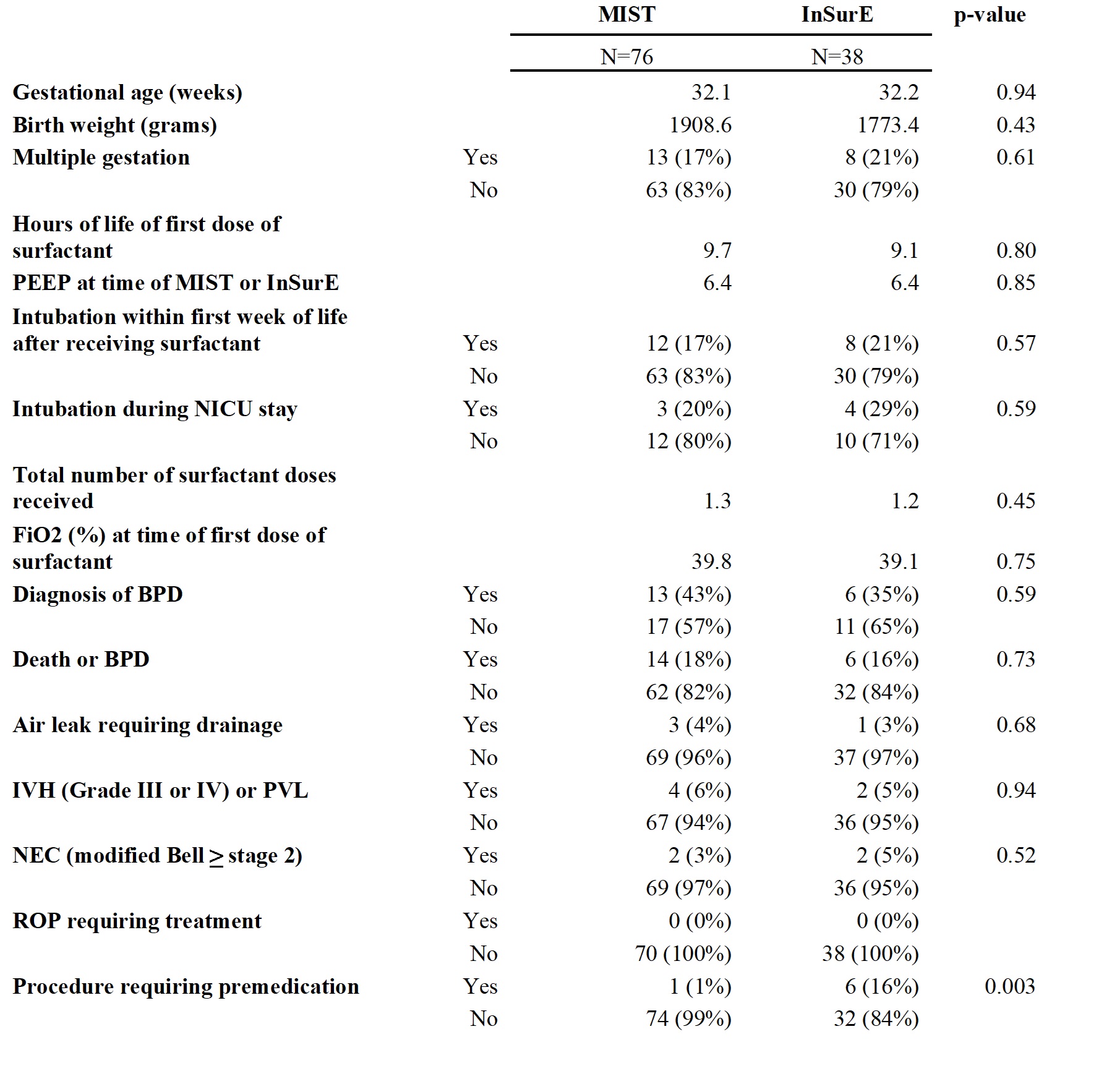 Mean is shown for gestational age, birth weight, hours of life of first dose of surfactant, PEEP at time of MIST or InSurE, total number surfactant doses received and FiO2 (%) at time of first dose of surfactant.
Mean is shown for gestational age, birth weight, hours of life of first dose of surfactant, PEEP at time of MIST or InSurE, total number surfactant doses received and FiO2 (%) at time of first dose of surfactant. 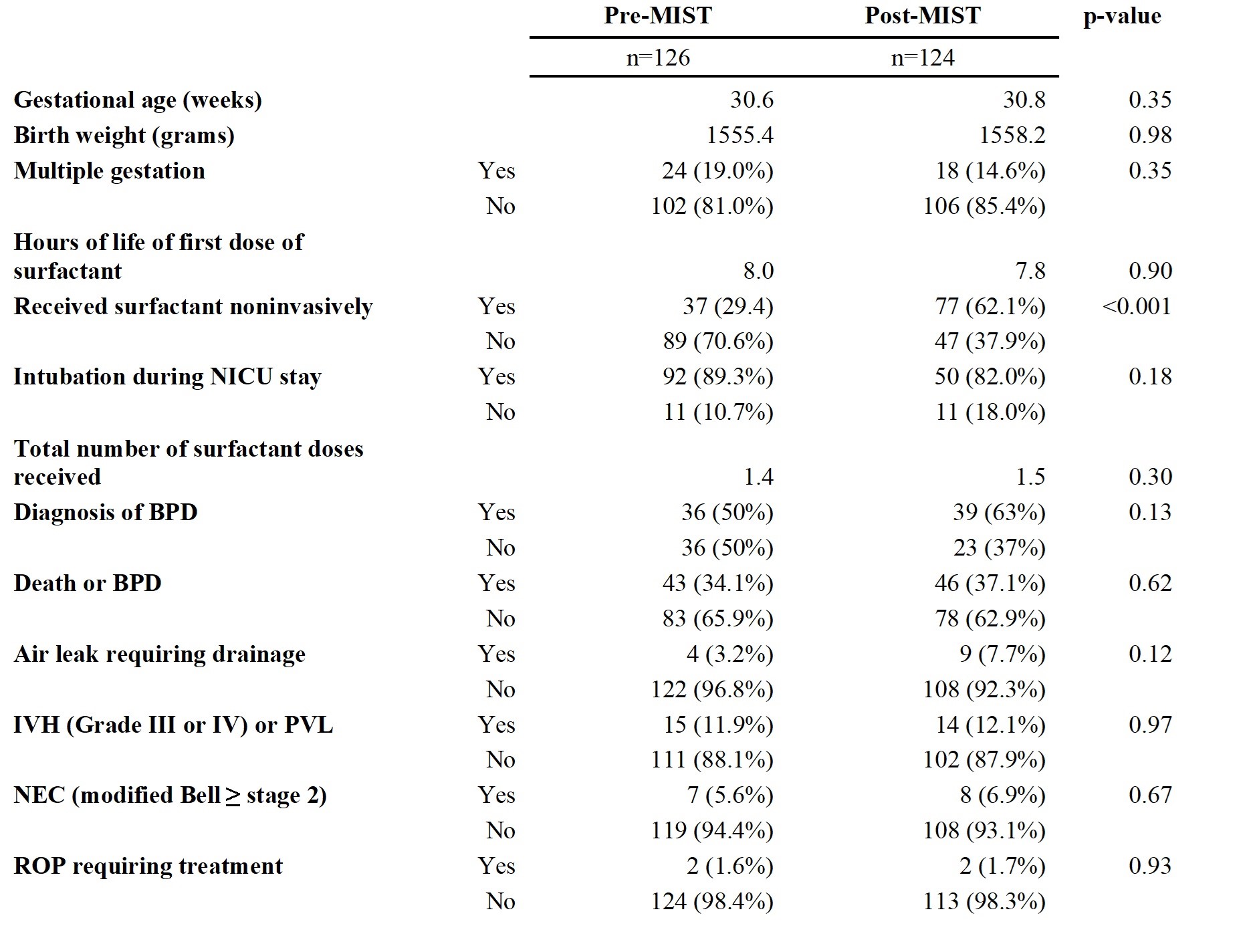 Mean is shown for gestational age, birth weight, hours of life at first dose of surfactant, and total number of surfactant doses received.
Mean is shown for gestational age, birth weight, hours of life at first dose of surfactant, and total number of surfactant doses received.