
Neonatal General 1: Respiratory, BPD
Session: Neonatal General 1: Respiratory, BPD
 photo")
Cindy T. McEvoy, MD, MCR (she/her/hers)
Professor of Pediatrics
Oregon Health & Science University School of Medicine
Portland, Oregon, United States
.jpg) Table
Table.jpg) Volcano plot of results from metabolome-wide association study (MWAS) using ANCOVA comparing blood metabolite levels between stable infants randomized to extended vs. discontinued CPAP (eCPAP -v- dCPAP). Individual dots represent a single metabolite colored by super pathway. Dots above the dashed red line represent metabolites that differed by randomized treatment group at p<0.05. The data shows there are multiple metabolites whose levels are significantly different between eCPAP and dCPAP.
Volcano plot of results from metabolome-wide association study (MWAS) using ANCOVA comparing blood metabolite levels between stable infants randomized to extended vs. discontinued CPAP (eCPAP -v- dCPAP). Individual dots represent a single metabolite colored by super pathway. Dots above the dashed red line represent metabolites that differed by randomized treatment group at p<0.05. The data shows there are multiple metabolites whose levels are significantly different between eCPAP and dCPAP.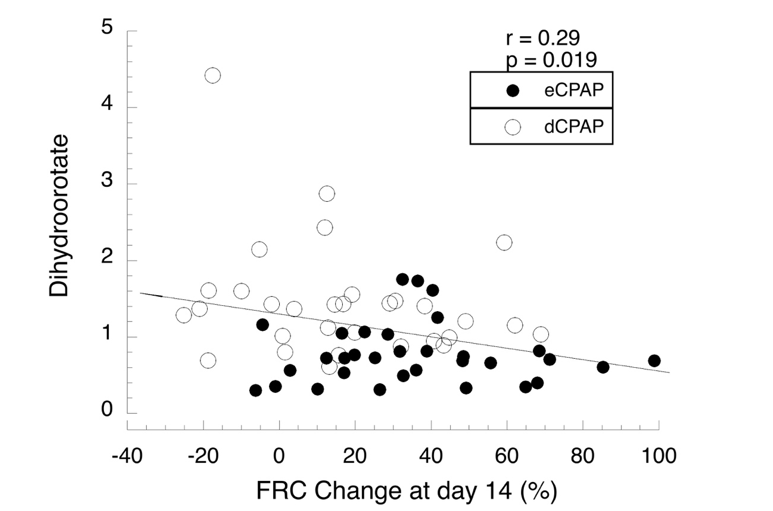 Regression analysis for blood levels of dihydroorotate, a precursor for de novo pyrimidine synthesis vs change in FRC for all 64 infants. Levels of metabolites were compared by ANCOVA and linear regression. TableVolcano plot of results from metabolome-wide association study (MWAS) using ANCOVA comparing blood metabolite levels between stable infants randomized to extended vs. discontinued CPAP (eCPAP -v- dCPAP). Individual dots represent a single metabolite colored by super pathway. Dots above the dashed red line represent metabolites that differed by randomized treatment group at p<0.05. The data shows there are multiple metabolites whose levels are significantly different between eCPAP and dCPAP.Regression analysis for blood levels of dihydroorotate, a precursor for de novo pyrimidine synthesis vs change in FRC for all 64 infants. Levels of metabolites were compared by ANCOVA and linear regression.
Regression analysis for blood levels of dihydroorotate, a precursor for de novo pyrimidine synthesis vs change in FRC for all 64 infants. Levels of metabolites were compared by ANCOVA and linear regression. TableVolcano plot of results from metabolome-wide association study (MWAS) using ANCOVA comparing blood metabolite levels between stable infants randomized to extended vs. discontinued CPAP (eCPAP -v- dCPAP). Individual dots represent a single metabolite colored by super pathway. Dots above the dashed red line represent metabolites that differed by randomized treatment group at p<0.05. The data shows there are multiple metabolites whose levels are significantly different between eCPAP and dCPAP.Regression analysis for blood levels of dihydroorotate, a precursor for de novo pyrimidine synthesis vs change in FRC for all 64 infants. Levels of metabolites were compared by ANCOVA and linear regression. 