
Neonatal Neurology 1
Session: Neonatal Neurology 1

Mohamed El-Dib, MD
Associate Professor of Pediatrics
Brigham and Women's Hospital / Harvard Medical School
Boston, Massachusetts, United States
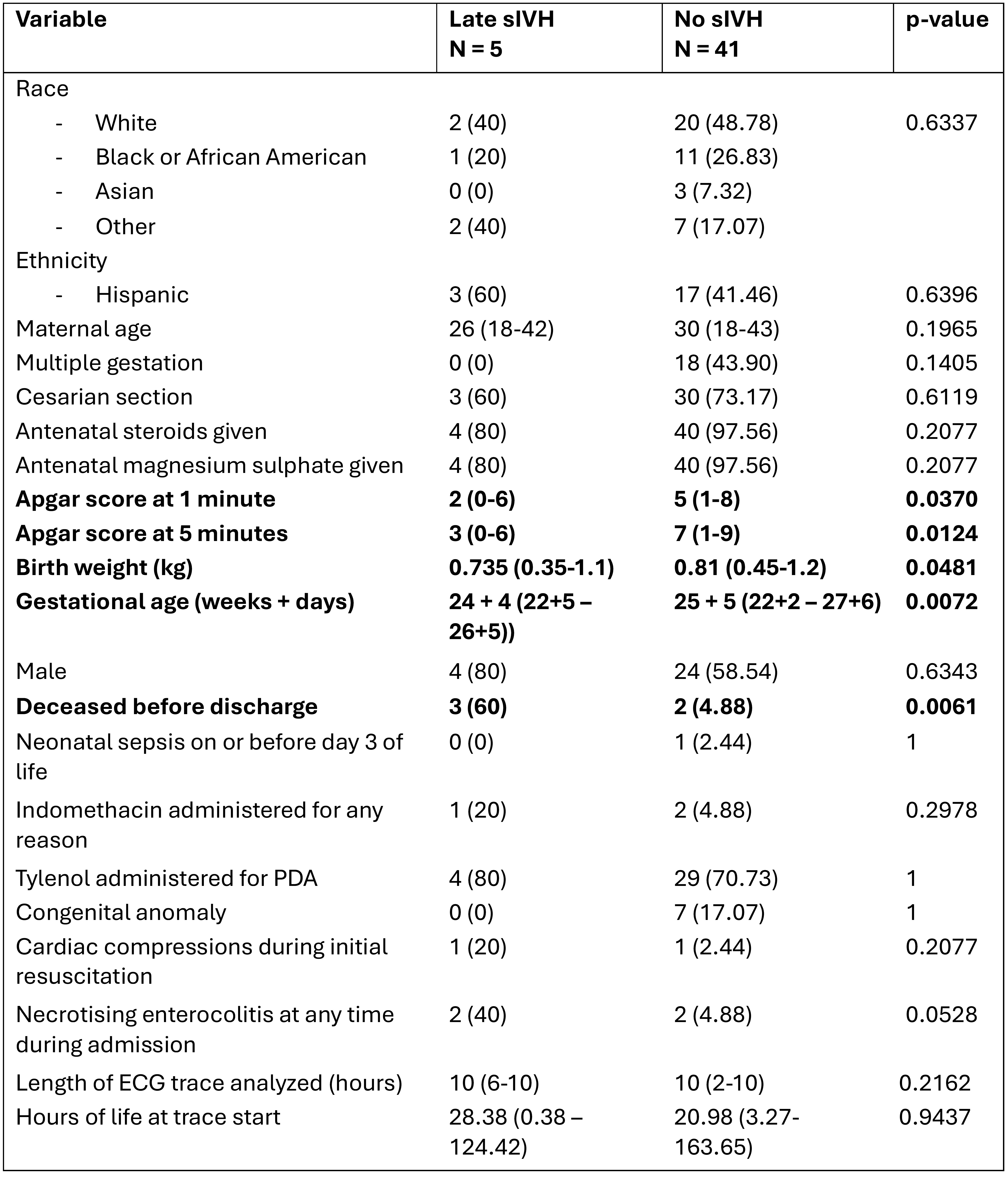 Statistical analysis of demographic data was carried out using Wilcoxon rank sum or 2 test (Fisher’s exact for variables with cell counts 5 or < 5) for continuous and categorical variables, respectively. No sIVH group also includes infants with low grade IVH (grades I and II).
Statistical analysis of demographic data was carried out using Wilcoxon rank sum or 2 test (Fisher’s exact for variables with cell counts 5 or < 5) for continuous and categorical variables, respectively. No sIVH group also includes infants with low grade IVH (grades I and II)..jpg) Each infant is represented by one dot. Pink denotes infants without sIVH and blue denotes infants with sIVH. The horizontal line represents the median value for each category. Analysis was carried out using Wilcoxon rank sum test with FDR adjustment. Threshold for significance was 0.05. * denotes p < 0.05, ** denotes p < 0.01, and ns denotes results that were not significant.
Each infant is represented by one dot. Pink denotes infants without sIVH and blue denotes infants with sIVH. The horizontal line represents the median value for each category. Analysis was carried out using Wilcoxon rank sum test with FDR adjustment. Threshold for significance was 0.05. * denotes p < 0.05, ** denotes p < 0.01, and ns denotes results that were not significant. 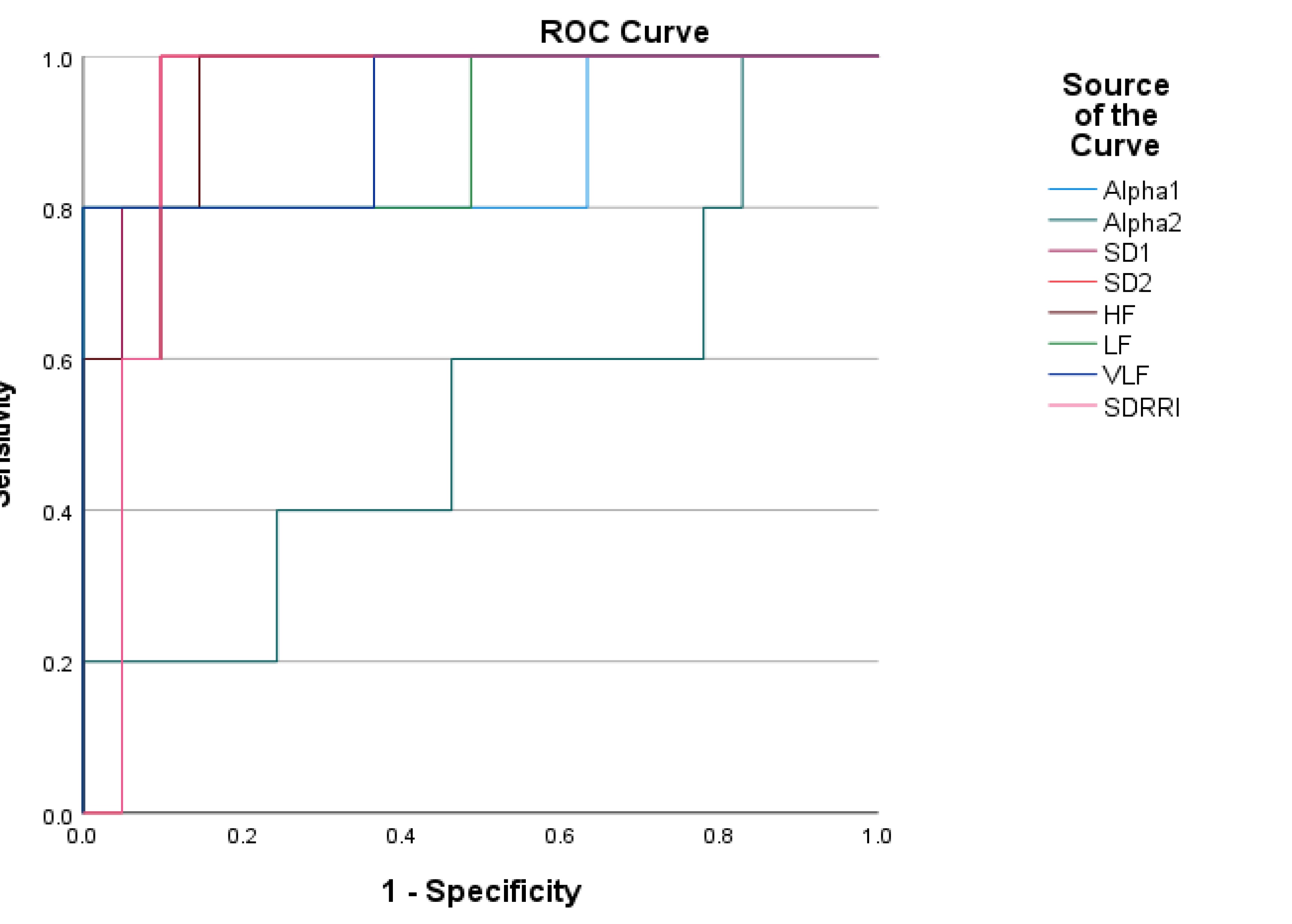 The source of the curve is given in the legend on the right-hand-side. In order of performance, the AUCs were SD1 (0.971), HF (0.951), SD2 and SDRRI (both 0.932), VLF (0.927), LF (0.902), alpha1 (0.873) and alpha2 (0.537).
The source of the curve is given in the legend on the right-hand-side. In order of performance, the AUCs were SD1 (0.971), HF (0.951), SD2 and SDRRI (both 0.932), VLF (0.927), LF (0.902), alpha1 (0.873) and alpha2 (0.537).