
Neonatal General 1: Respiratory, BPD
Session: Neonatal General 1: Respiratory, BPD
 photo")
Tejeshwar S. Sangha, MD (he/him/his)
Resident PGY2
Eastern Virginia Medical School/ODU Health Sciences
Norfolk, Virginia, United States
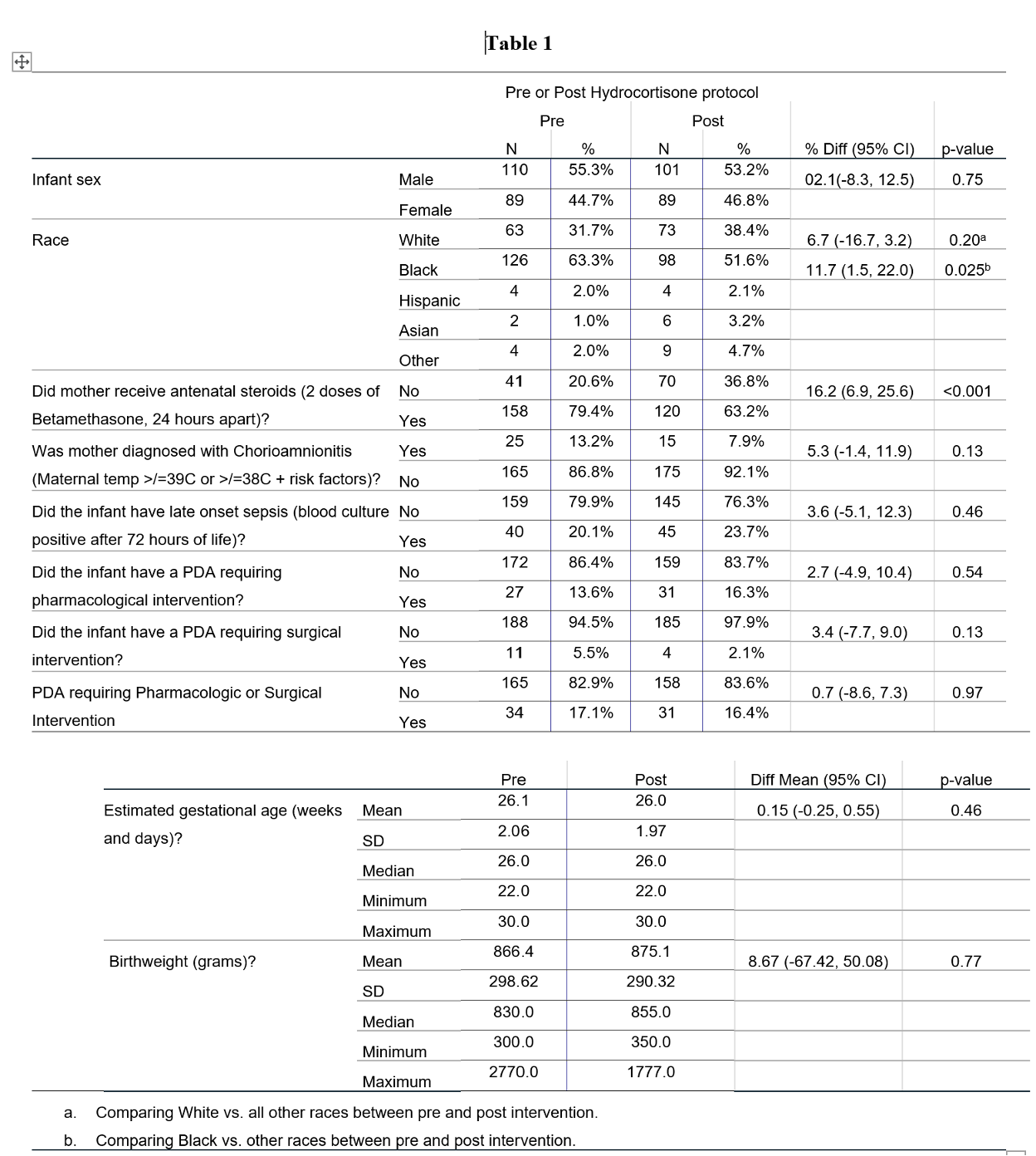 Baseline Characteristics
Baseline Characteristics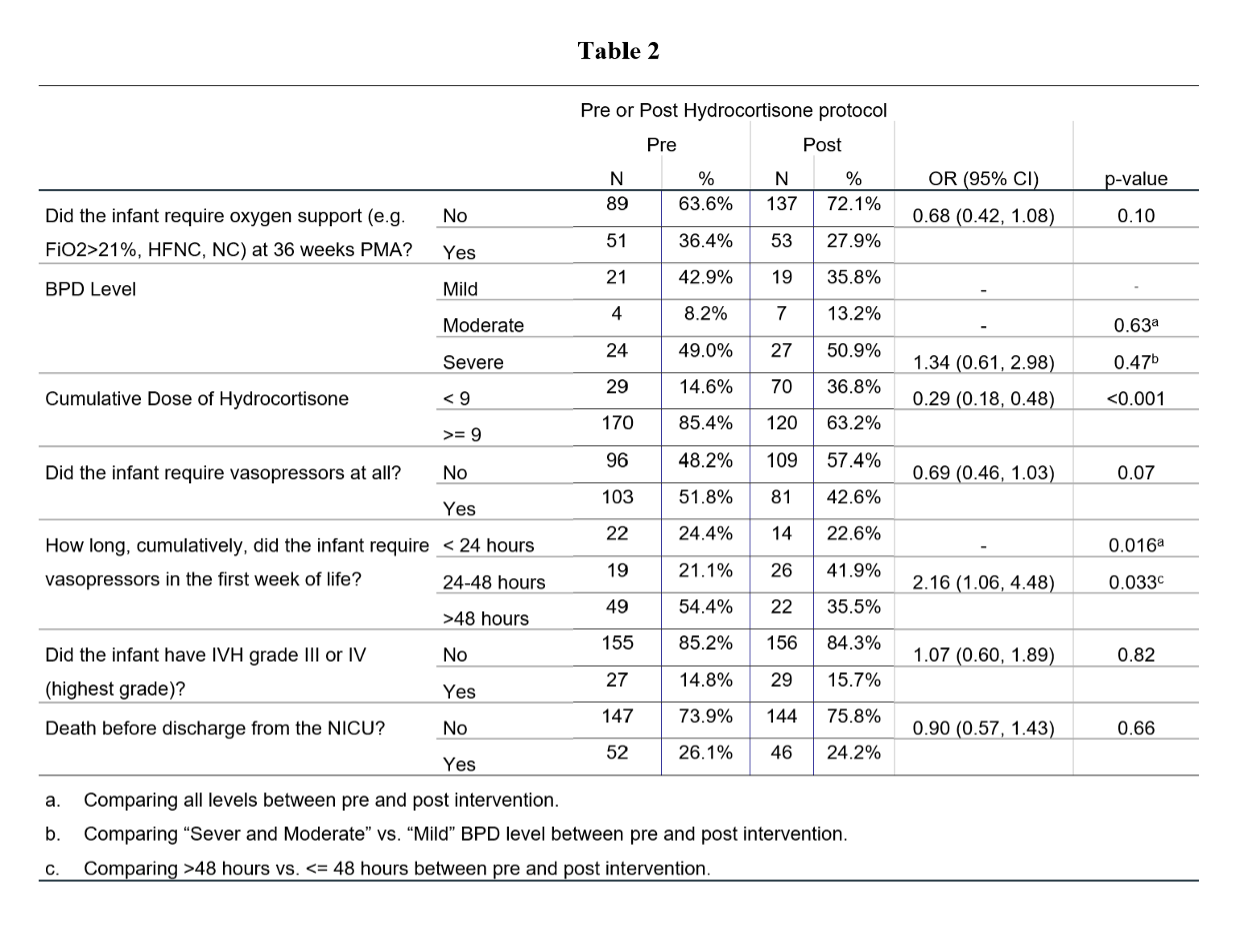 Primary outcomes
Primary outcomes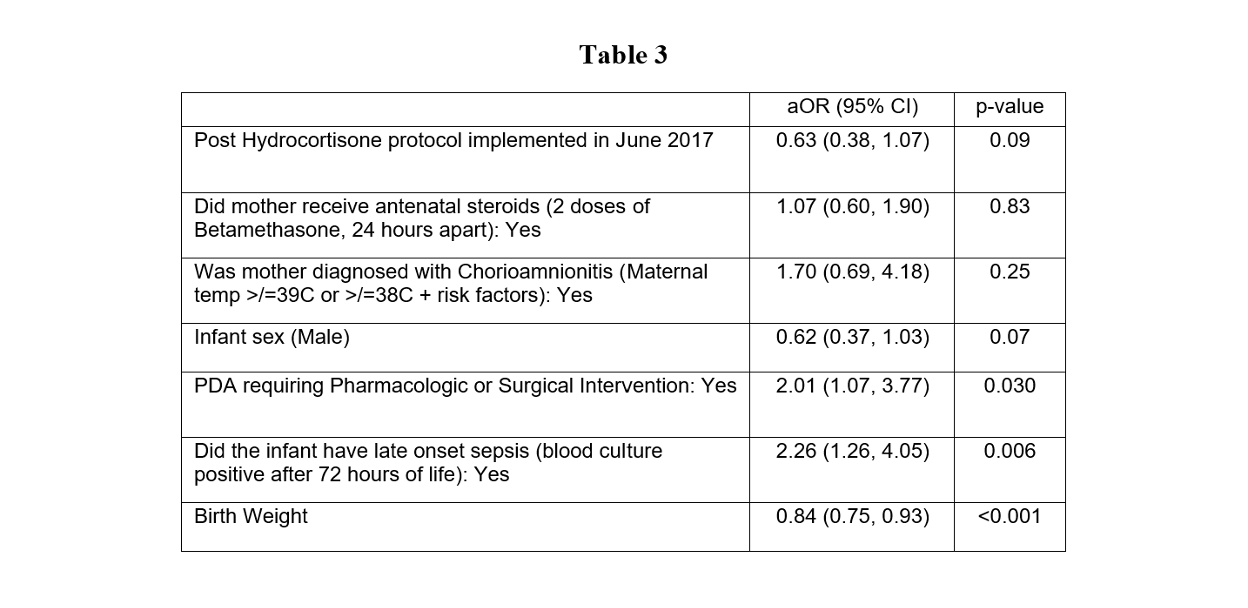 Odds of being diagnosed with BPD
Odds of being diagnosed with BPD