
Neonatal/Infant Resuscitation 1
Session: Neonatal/Infant Resuscitation 1
 (she/her/hers) photo")
Paige J. Riddington, BSc(Hons) (she/her/hers)
PhD Student
Monash University
Clayton, Victoria, Australia
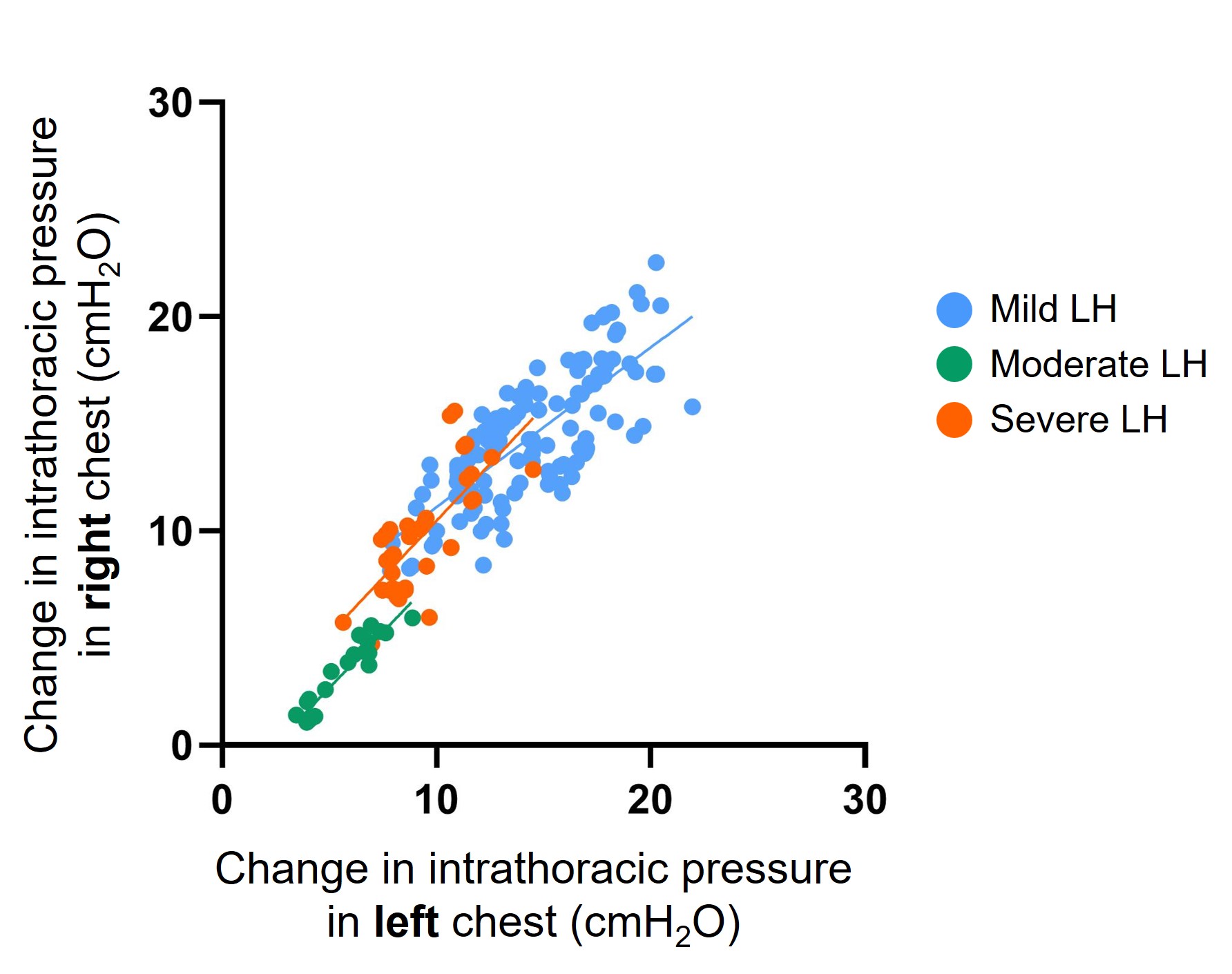 SB DH lambs with mild lung hypoplasia had a spontaneous repair of the diaphragmatic defect (closed defect). SB DH lambs with moderate and severe DH had a patent (open) defect. Intrathoracic pressure was measured with a saline filled latex balloon tipped catheter placed within the left and right intrapleural space of each lamb.
SB DH lambs with mild lung hypoplasia had a spontaneous repair of the diaphragmatic defect (closed defect). SB DH lambs with moderate and severe DH had a patent (open) defect. Intrathoracic pressure was measured with a saline filled latex balloon tipped catheter placed within the left and right intrapleural space of each lamb.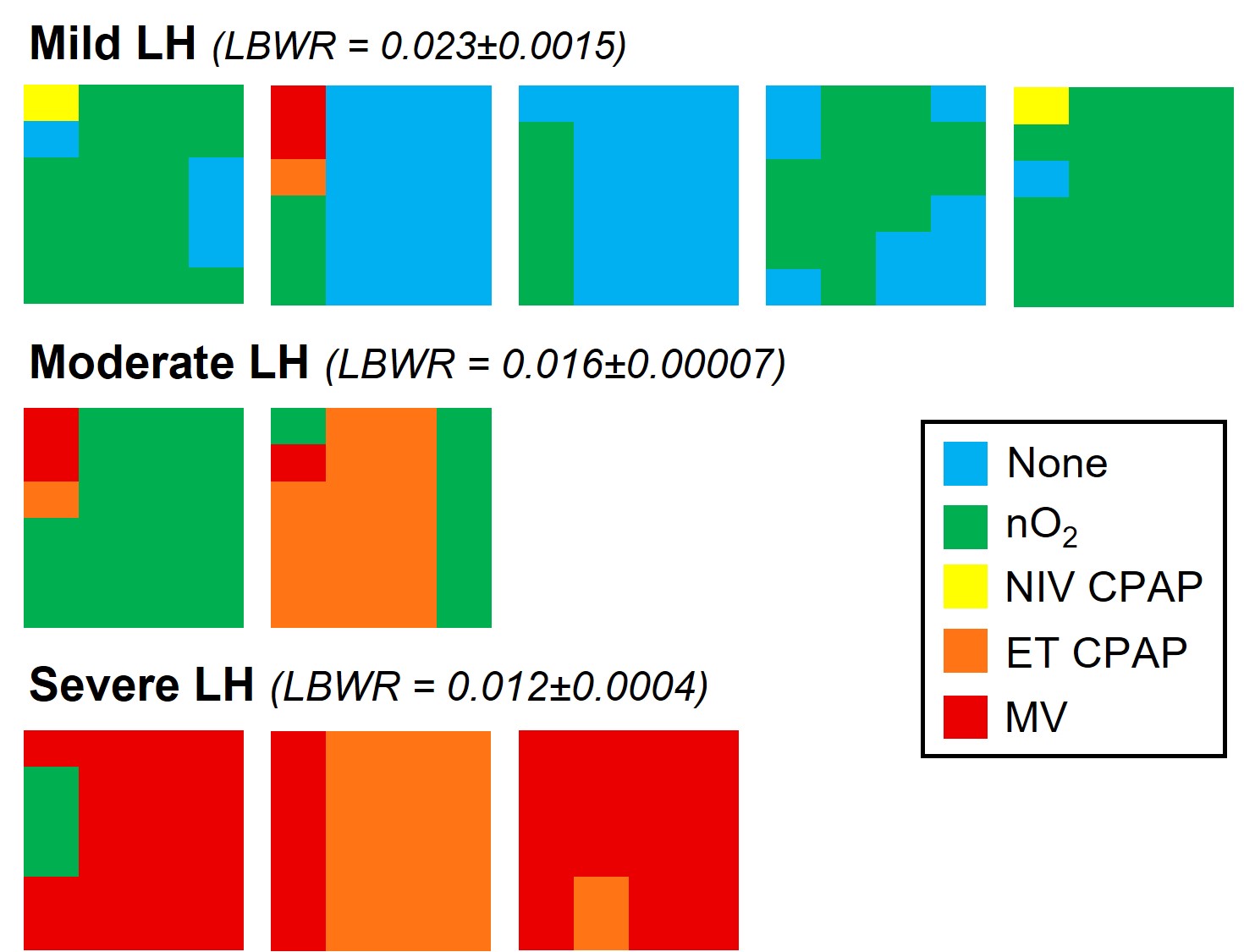 Types of respiratory support graded according to decreasing intensity of support. Blue = no respiratory support, Green = nasal gas flow (with oxygen; nO2), Yellow = Non-invasive CPAP (delivered via face mask or laryngeal mask; NIV CPAP), Orange = intubated with continuous positive airway pressure (ET CPAP), Red = Intubated with mechanical ventilation (MV). Individual lambs with Mild LH, Moderate LH and Severe LH are presented in left-to-right in order of delivery. The 2 hours of respiratory support are represented in columns from left to right with each column presenting the proportion of time spent on any form of respiratory support for that 30-minute interval. LH = lung hypoplasia, LBWR = lung-to-body weight ratio (a proxy for LH; healthy lungs = 0.033±0.004).
Types of respiratory support graded according to decreasing intensity of support. Blue = no respiratory support, Green = nasal gas flow (with oxygen; nO2), Yellow = Non-invasive CPAP (delivered via face mask or laryngeal mask; NIV CPAP), Orange = intubated with continuous positive airway pressure (ET CPAP), Red = Intubated with mechanical ventilation (MV). Individual lambs with Mild LH, Moderate LH and Severe LH are presented in left-to-right in order of delivery. The 2 hours of respiratory support are represented in columns from left to right with each column presenting the proportion of time spent on any form of respiratory support for that 30-minute interval. LH = lung hypoplasia, LBWR = lung-to-body weight ratio (a proxy for LH; healthy lungs = 0.033±0.004).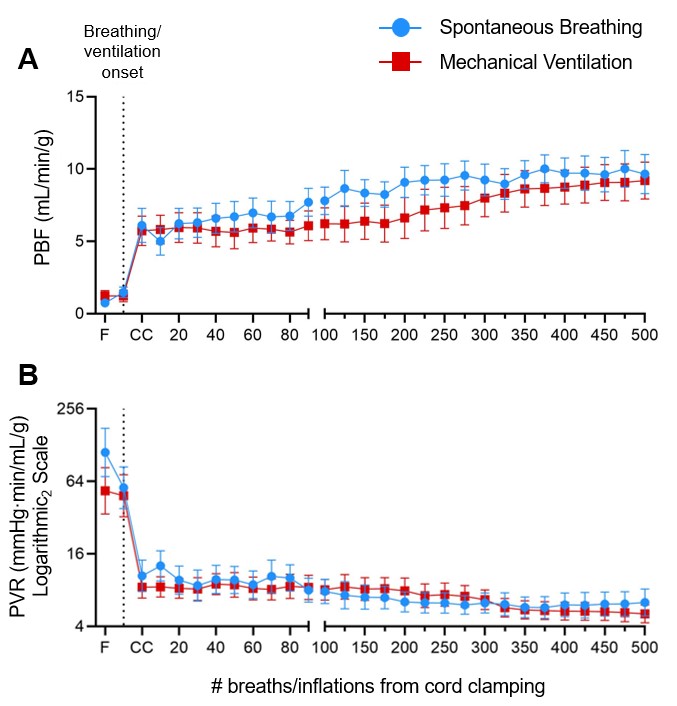 Pulmonary blood flow (PBF; A) and pulmonary vascular resistance (PVR; B) corrected for left lung weight in SB DH lambs (n=10) and MV DH lambs (n=9). Data expressed as mean±SEM. F = Fetal, CC = Cord clamping, PVR = (pulmonary artery pressure – left atrial pressure)/pulmonary blood flow.
Pulmonary blood flow (PBF; A) and pulmonary vascular resistance (PVR; B) corrected for left lung weight in SB DH lambs (n=10) and MV DH lambs (n=9). Data expressed as mean±SEM. F = Fetal, CC = Cord clamping, PVR = (pulmonary artery pressure – left atrial pressure)/pulmonary blood flow. 