
Neonatal General 2: Neurology
Session: Neonatal General 2: Neurology

Trisha Mulamreddy, MD/MPH
Resident
University of California Davis Children's Hospital
Sacramento, California, United States
.png) Comparison of pregnancy, delivery and neonatal outcomes between inborn and outborn infants with HIE treated with TH
Comparison of pregnancy, delivery and neonatal outcomes between inborn and outborn infants with HIE treated with TH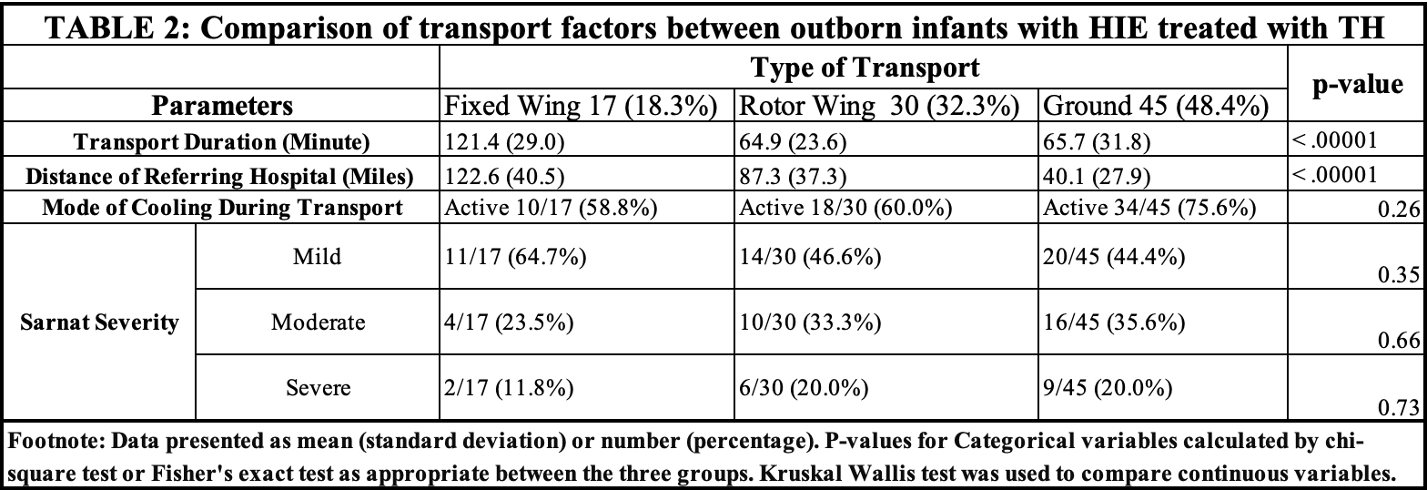 Comparison of transport factors between outborn infants with HIE treated with TH
Comparison of transport factors between outborn infants with HIE treated with TH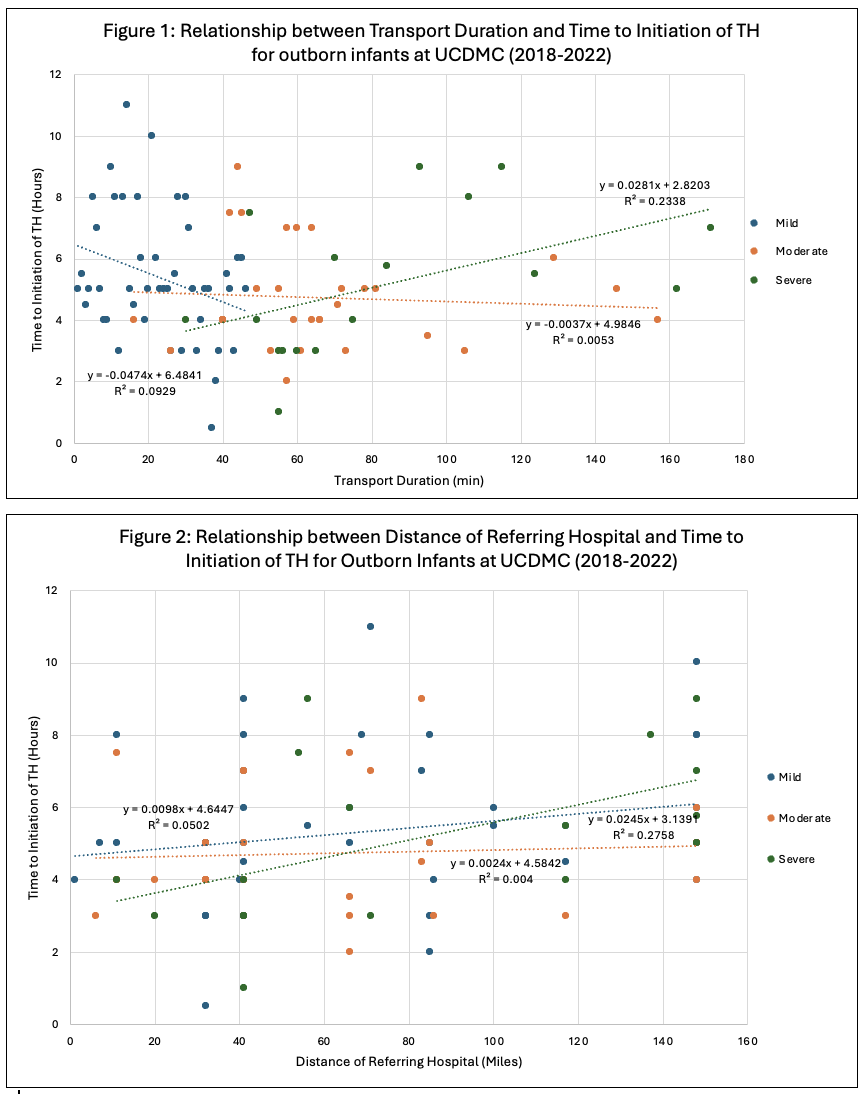 Relationship between transport duration, Sarnat severity, and distance of referring hospital with timing of initiation of TH for outborn infants with HIE.
Relationship between transport duration, Sarnat severity, and distance of referring hospital with timing of initiation of TH for outborn infants with HIE.