
Neonatal Neurology 3
Session: Neonatal Neurology 3
Yangming Ou, PhD
Associate Professor
Boston Children's Hospital
Boston, Massachusetts, United States
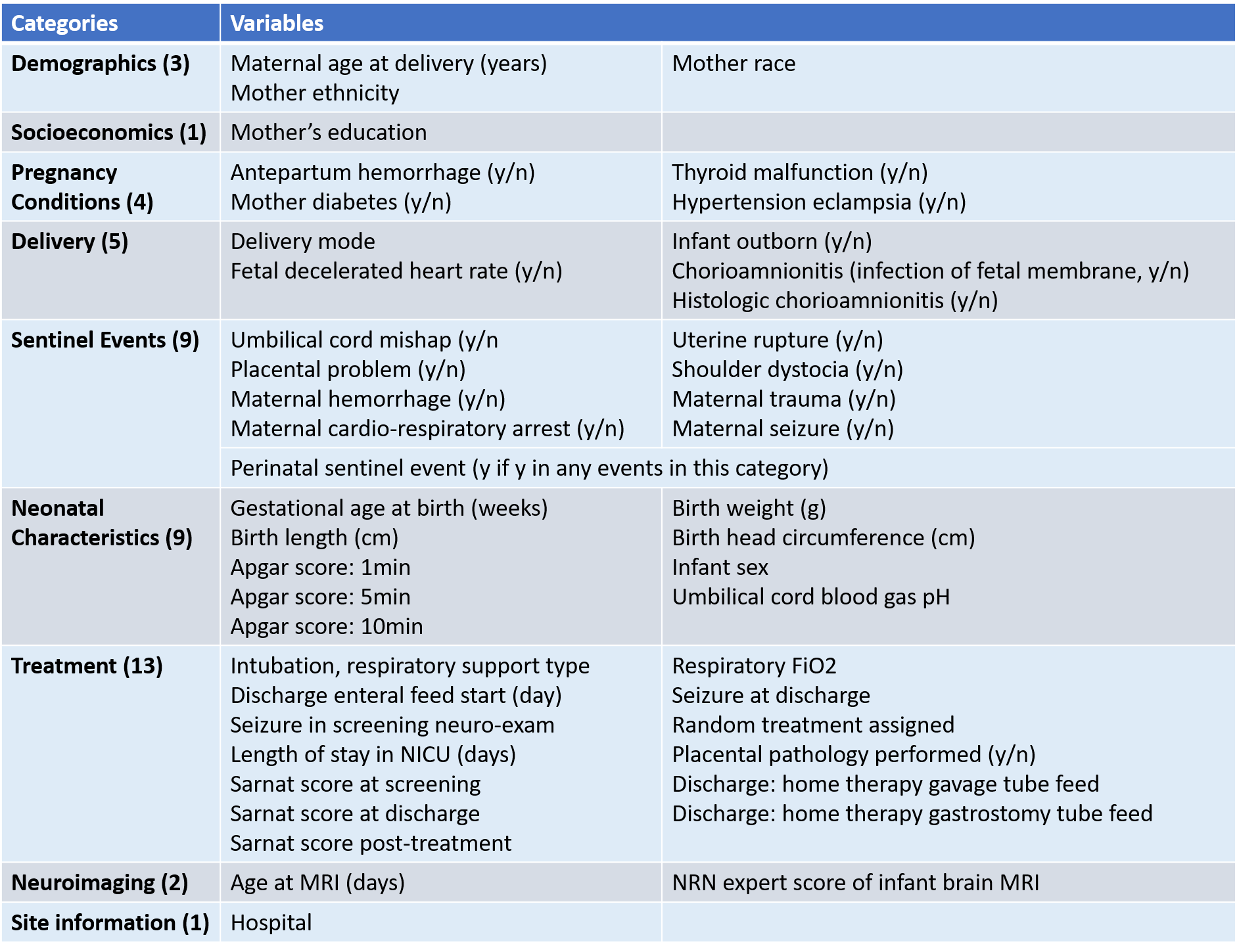 Table 1. The 47 clinical and MRI variables we have included as predictors in this study.
Table 1. The 47 clinical and MRI variables we have included as predictors in this study. 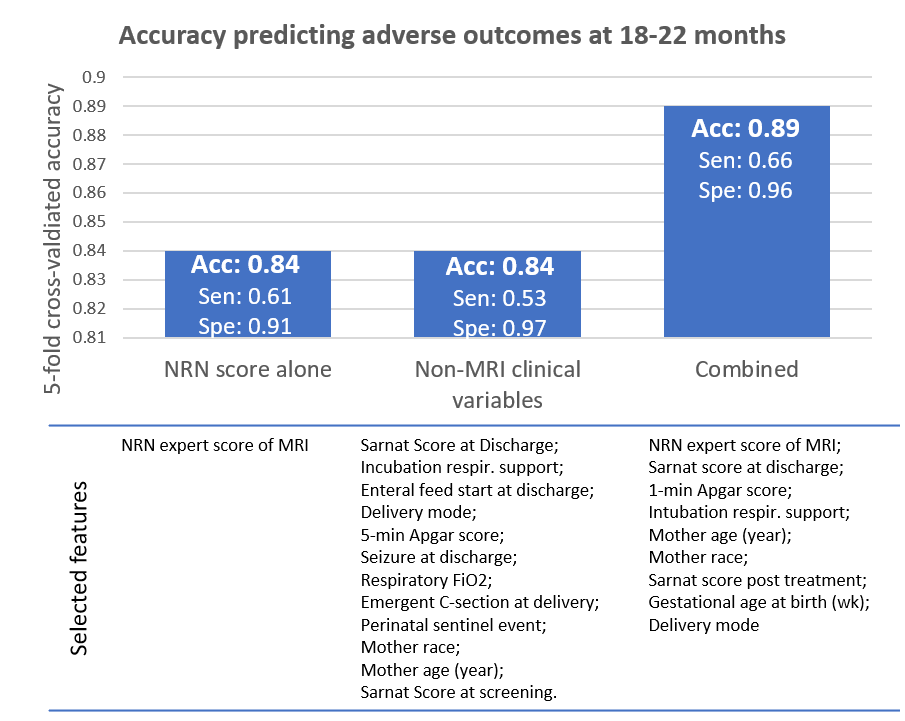 Fig 1. Accuracies and auto-selected variables in three experiments for outcome prediction.
Fig 1. Accuracies and auto-selected variables in three experiments for outcome prediction.