
Neonatal Neurology 3
Session: Neonatal Neurology 3
 photo")
Marie T. Berg, MD (she/her/hers)
Clinical Associate Professor
University Of Florida
University Of Florida College Of Medicine, Florida, United States
.png)
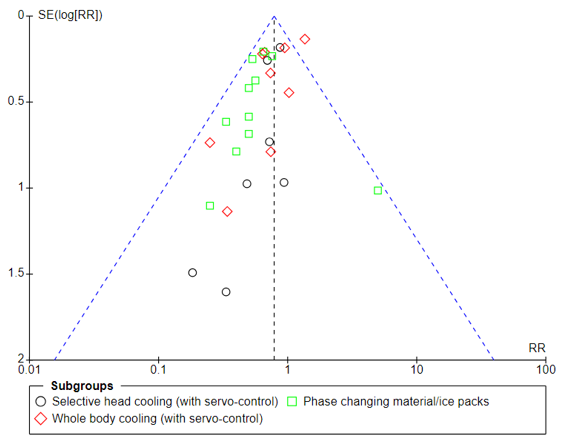 Mortality reported at last follow-up in all infants (all trials)
Mortality reported at last follow-up in all infants (all trials)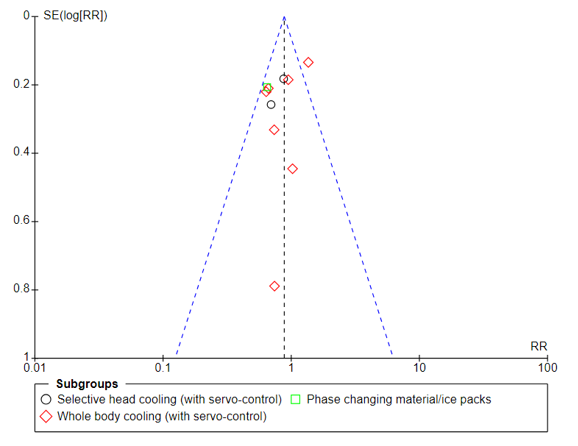 Mortality reported at last follow-up in all infants (multicenter trials)
Mortality reported at last follow-up in all infants (multicenter trials)