
Neonatal Quality Improvement 6
Session: Neonatal Quality Improvement 6
 Credit")
Navin Bhopal, MD (he/him/his)
Neonatologist
Phoenix Children's Hospital
Phoenix, Arizona, United States
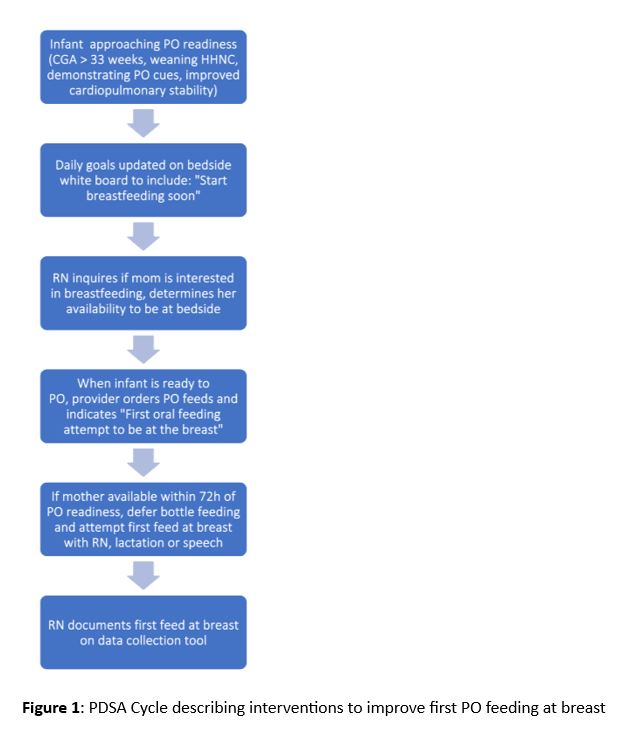 PDSA Cycle describing interventions to improve first PO feeding at breast
PDSA Cycle describing interventions to improve first PO feeding at breast.jpg) Run chart describing rates of first oral feeds at breast. The median rate of first oral feeds at breast was 40%. We introduced a systematic approach to first initiate the first PO feed at breast in November 2023 and saw a statistical shift in our breastfeeding rate starting in February 2024. In September 2024, we altered our data collection method to improve accuracy.
Run chart describing rates of first oral feeds at breast. The median rate of first oral feeds at breast was 40%. We introduced a systematic approach to first initiate the first PO feed at breast in November 2023 and saw a statistical shift in our breastfeeding rate starting in February 2024. In September 2024, we altered our data collection method to improve accuracy.