
Neonatal Hemodynamics and Cardiovascular Medicine 3
Session: Neonatal Hemodynamics and Cardiovascular Medicine 3
 photo")
Aisling M. Smith, PhD (she/her/hers)
Doctor
The Rotunda Hospital
Dublin, Dublin, Ireland
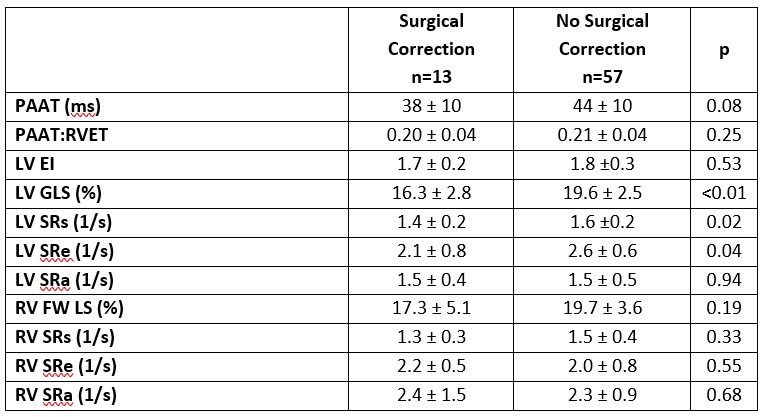 Values are presented as means (SD). A p value < 0.05 was considered significant.
Values are presented as means (SD). A p value < 0.05 was considered significant.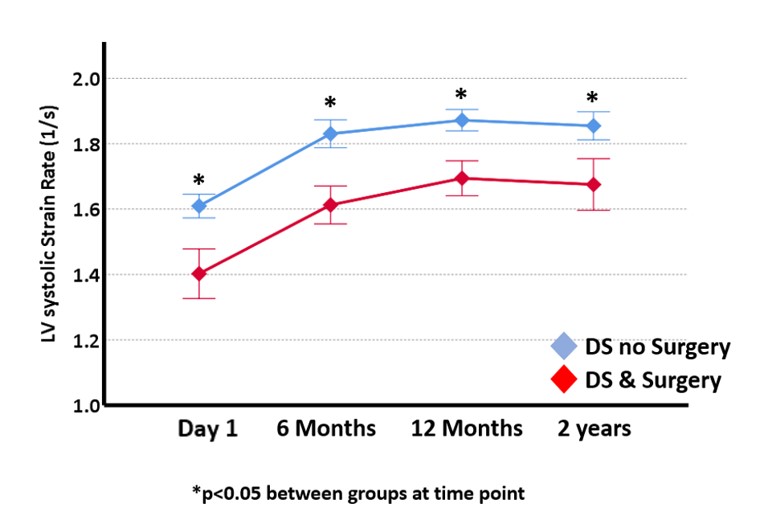 Values are presented as mean and standard error. DS: Down syndrome; LV: left ventricle.
Values are presented as mean and standard error. DS: Down syndrome; LV: left ventricle.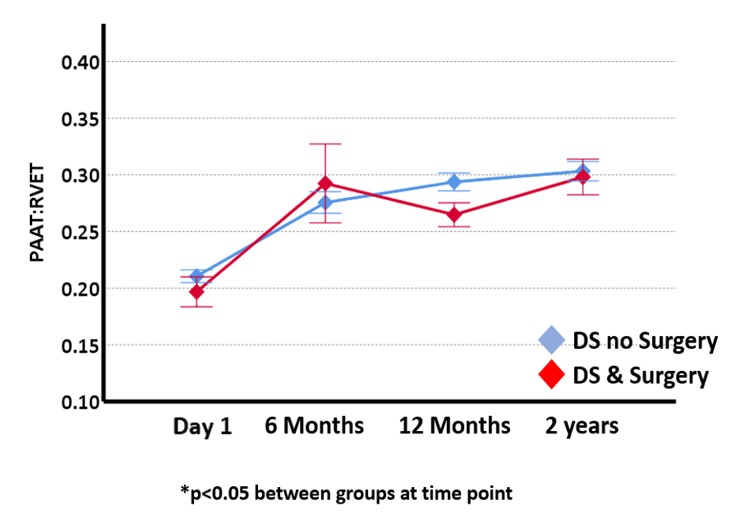 Values are presented as mean and standard error. DS: Down syndrome; PAAT: pulmonary artery acceleration time; RVET: right ventricular ejection time.
Values are presented as mean and standard error. DS: Down syndrome; PAAT: pulmonary artery acceleration time; RVET: right ventricular ejection time. 