
Neonatal Quality Improvement 5
Session: Neonatal Quality Improvement 5
 Credit")
 photo")
Darah Yuhas, MD (she/her/hers)
Neonatal-Perinatal Fellow
Johns Hopkins All Children's Hospital
Tampa, Florida, United States
.png) Key driver diagram for increasing time spent at goal oxygen saturation, linking change ideas to primary drivers.
Key driver diagram for increasing time spent at goal oxygen saturation, linking change ideas to primary drivers.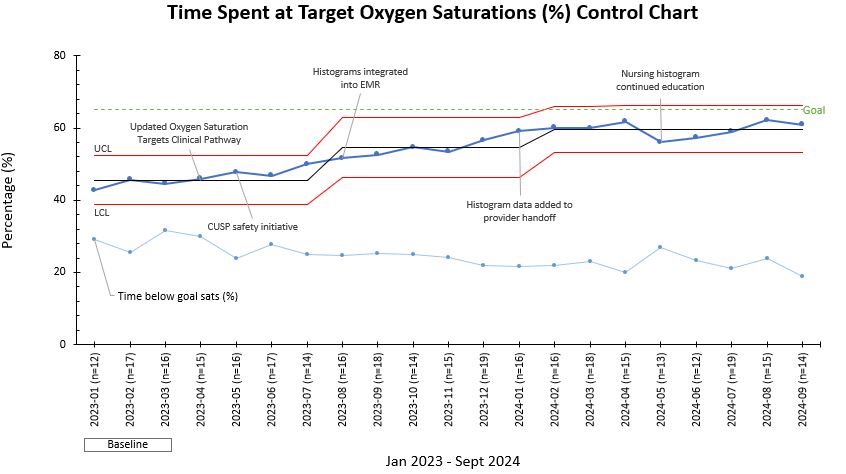 Control chart displaying average monthly time spent at goal oxygen saturation in VLBW infants requiring oxygen from January 2023
Control chart displaying average monthly time spent at goal oxygen saturation in VLBW infants requiring oxygen from January 2023 .jpg) A, Control chart displaying average monthly alarm limits set accurately in VLBW infants requiring oxygen from January 2023 through September 2024. Red lines indicate the upper control limit and lower control limit. The center line (mean) was adjusted after special
A, Control chart displaying average monthly alarm limits set accurately in VLBW infants requiring oxygen from January 2023 through September 2024. Red lines indicate the upper control limit and lower control limit. The center line (mean) was adjusted after special