Medical Education 3: Simulation
Session: Medical Education 3: Simulation
 photo")
Carissa Bunke, MD (she/her/hers)
Pediatric Emergency Medicine Faculty
Children's Hospitals and Clinics of Minnesota
Inver Grove Heights, Minnesota, United States
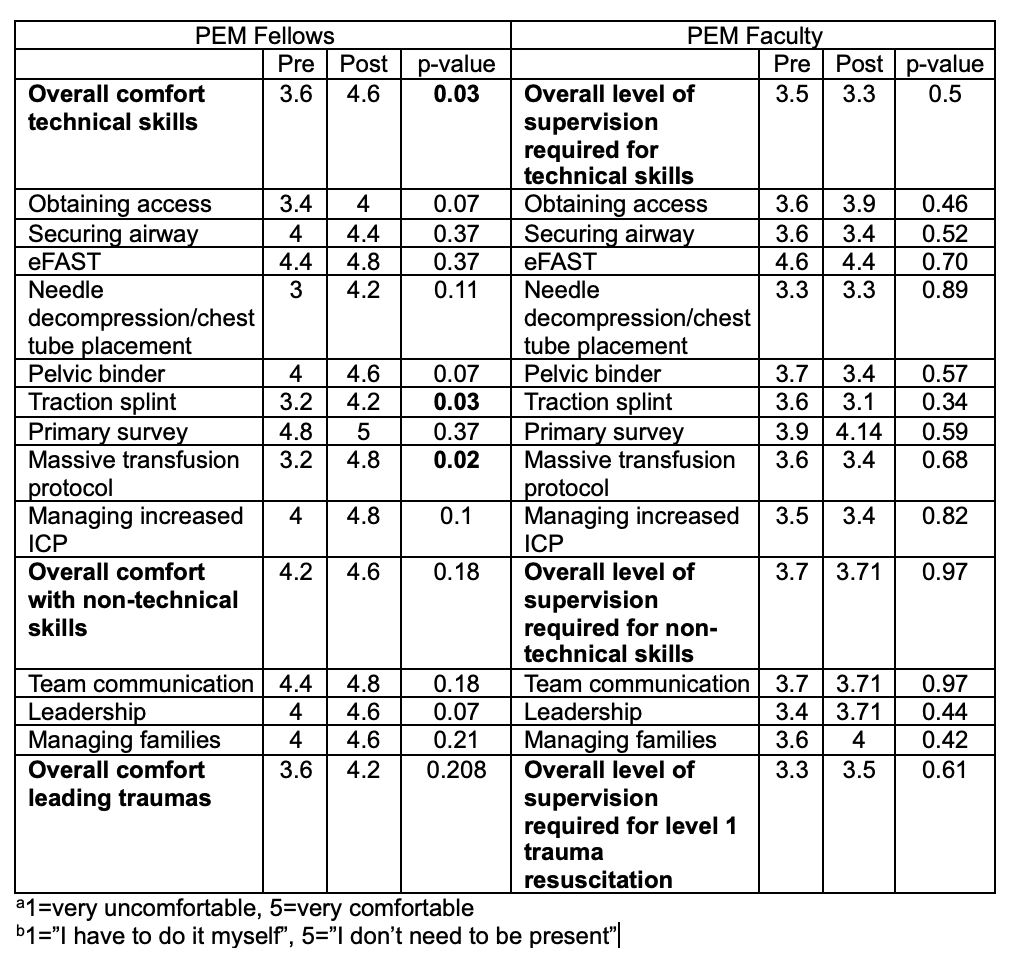
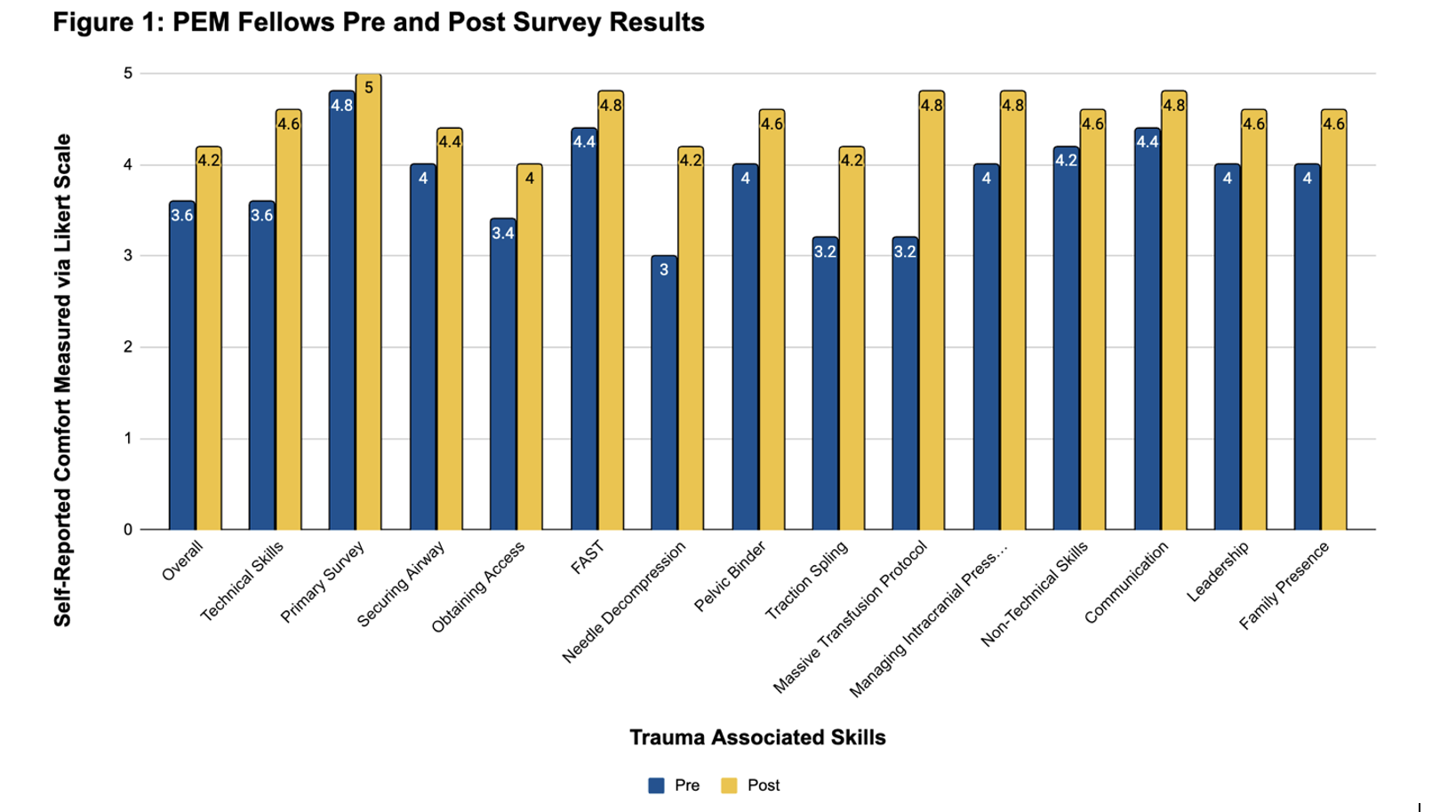 Results of PEM Fellows pre and post-implementation survey. Fellows rated their self-reported comfort in various aspects of trauma resuscitations on a Likert scale. Results were averaged and compared via a paired T-test. There was statistically significant improvement (p <0.05) in overall technical skills, traction splint application, and initiating massive transfusion protocol.
Results of PEM Fellows pre and post-implementation survey. Fellows rated their self-reported comfort in various aspects of trauma resuscitations on a Likert scale. Results were averaged and compared via a paired T-test. There was statistically significant improvement (p <0.05) in overall technical skills, traction splint application, and initiating massive transfusion protocol.